Introduction
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Prenatal
- Pathology: Teratogenic
- Rarity Classification: Rare
- Typical Onset: Infancy
- Gender Impact: Mostly Women
- Seizure Prevalence: Minority (10-50%)
- Population Trend: Decreasing
Pathophysiology
Possible implication of 3q24.3, 6p25, 13q32.2-33.2 or 9p, but doesn't seem to be heritable so probably secondary to teroatogenetics.
AAC Considerations
Recommended Access Modalities: All - Variable
Additional Clinical Notes
A specific type of prenatal abnormal development of t he cerebellum. Very often comorbid with other syndromes, particularly chromosomal disorders, so viewing this is as its own population is problematic.
Patient Advocacy & Support Organizations
Quick Reference
| Metric | Value |
|---|---|
| Incidence | 1 in 25,000 to 35,000 live births |
| Prevalence | 6.79 per 100,000 births (European data); 2.74 per 100,000 livebirths |
| Age of Onset | Birth to early infancy (symptoms vary) |
| AT Required | 50-70% require assistive technology depending on severity |
Dandy-Walker Syndrome
Formal Name: Dandy-Walker Malformation
Demographic Information
- Incidence: Approximately 1 in 25,000 to 35,000 live births.
- Prevalence: Rare, with varying estimates of global prevalence.
- Gender: Affects both males and females equally.
- Onset Age: Symptoms can be present at birth or become noticeable within the first year of life; some cases are diagnosed prenatally via ultrasound.
Coding
- ICD-11: LD48.3
- ICD-10-CM: Q03.1
- OMIM: 220200 - Dandy-Walker Malformation.
- UMLS: C0011029 - Dandy-Walker Malformation.
- MeSH: D019527 - Dandy-Walker Syndrome.
- GARD: 11708 - Dandy-Walker Malformation.
Medical Features and Pathophysiology
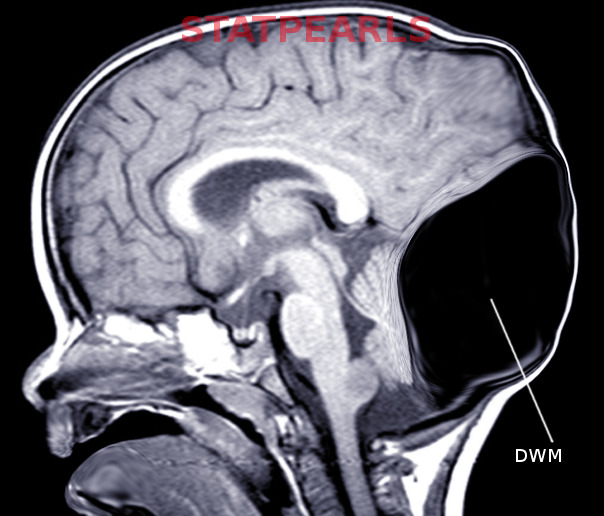
- Etiology: Dandy-Walker Syndrome (DWS) is a congenital brain malformation involving the cerebellum and the fluid-filled spaces around it. The exact cause is unknown, but it may involve genetic mutations or environmental factors during pregnancy, such as infections, toxin exposure, or maternal diabetes. Chromosomal abnormalities, such as trisomy 18, 13, and 21, are also associated with DWS.
- Pathology: DWS is characterized by hypoplasia (underdevelopment) or agenesis (absence) of the cerebellar vermis, cystic dilation of the fourth ventricle, and enlargement of the posterior fossa. These structural abnormalities can lead to hydrocephalus (excess fluid in the brain), increased intracranial pressure, and various neurological symptoms.
Symptoms
Infants and Young Children:
- Macrocephaly (large head size) due to hydrocephalus.
- Developmental delays, particularly in motor skills.
- Hypotonia (low muscle tone) and spasticity (stiff muscles).
- Poor coordination and balance issues.
- Signs of increased intracranial pressure such as irritability, vomiting, and bulging at the back of the skull.
- Seizures.
- Breathing abnormalities and jerky eye movements.
Older Children:
- Learning disabilities and intellectual impairment.
- Behavioral issues and mood swings.
- Difficulty with fine motor skills.
- Visual impairments and other sensory deficits.
- Progressive neurological decline in severe cases.
Diagnosis
Diagnosis is typically made through prenatal ultrasound or fetal MRI, which can reveal brain malformations. Postnatal diagnosis involves imaging studies such as MRI or CT scans to confirm the presence of characteristic features. Genetic testing may be recommended to identify any associated chromosomal abnormalities.
Assistive Suggestions and Requirements
Approximately 50-70% of individuals with Dandy-Walker Syndrome require assistive technology, depending on severity and comorbid conditions. Communication needs correlate with intellectual disability severity and motor impairment. Many individuals present with hypotonia and coordination deficits affecting motor access.
Assistive Technology Suggestions: - Mobility Aids: Customized wheelchairs and walkers to assist with balance and mobility. - Communication Devices: AAC devices for individuals with speech impairments. - Adaptive Educational Tools: Tablets and computers with specialized software to support learning. - Environmental Control Systems: Devices to control the home environment, enhancing independence.
Access Modalities: - Switch Access: Useful for individuals with limited motor control. - Eye-Gaze Technology: Enables control through eye movements for severe motor impairments. - Touchscreen Devices: Beneficial for individuals with some hand control.
Care Management and Therapeutic Techniques
- Aims:
- Hydrocephalus Management: Reducing intracranial pressure through surgical interventions such as ventriculoperitoneal (VP) shunts.
- Developmental Support: Maximizing potential through early intervention and continuous therapies focusing on cognitive, motor, and communication skills.
- Daily Living Assistance: Providing support for daily activities through the use of adaptive equipment and assistive technologies.
- Family Support: Offering resources, education, and emotional support to families, ensuring a nurturing and supportive environment.
- SLP Suggestions:
- Early Intervention: Initiating speech and language therapy as early as possible to support communication development. Programs should focus on basic communication skills, understanding, and social interactions.
- AAC Implementation: Introducing and training the use of AAC devices tailored to the individual’s needs and capabilities. Regular updates and customization of the device vocabulary ensure it remains relevant and useful.
- Oral Motor Therapy: Addressing feeding and swallowing difficulties through targeted exercises to improve oral motor function and safety. Techniques may include strengthening exercises, positioning strategies, and texture modifications.
- Family Training: Educating and involving family members in using AAC devices and communication strategies at home to ensure consistency and reinforcement. Providing resources and training sessions can empower families to support communication development effectively.
- Special Educator Suggestions:
- Individualized Education Plan (IEP): Developing and regularly updating an IEP that includes specific goals and accommodations tailored to the student's strengths and needs. The IEP should address cognitive, motor, communication, and social-emotional development.
- Sensory Integration Therapy: Incorporating sensory activities that help with sensory processing issues, improving focus and engagement. Activities may include tactile play, movement exercises, and proprioceptive input.
- Inclusive Classroom Strategies: Utilizing visual supports, structured routines, and differentiated instruction to create an inclusive learning environment. Strategies such as visual schedules, social stories, and task analysis can enhance understanding and participation.
- Life Skills Training: Emphasizing the development of life skills that promote independence and daily living activities. This includes teaching self-care skills, social interactions, and functional communication.
- Occupational Therapist Suggestions:
- Motor Skill Development: Implementing exercises and activities to improve fine and gross motor skills, enhancing overall physical functioning. Techniques may include hand strengthening exercises, coordination tasks, and mobility training.
- Adaptive Equipment: Recommending and training the use of adaptive equipment for daily tasks, such as specialized utensils, writing aids, and dressing aids. These tools can enhance independence and facilitate participation in daily activities.
- Sensory Processing: Addressing sensory processing issues through tailored sensory diets and activities that help regulate responses to sensory input. This may involve creating a sensory-friendly environment and incorporating sensory breaks into the daily routine.
- Positioning and Mobility: Ensuring proper positioning and support in wheelchairs and other seating systems to prevent deformities and promote comfort. Assessing and adapting the home and school environment to facilitate mobility and accessibility.
- Recommendations on AAC:
- Symbol-Based Communication: For individuals with limited verbal abilities, using symbol-based communication systems such as picture boards or symbol-based AAC devices can be highly effective. These systems use visual symbols to represent words or concepts, facilitating communication.
- Text-Based Communication: For those who can read and write, text-based AAC devices can provide a more reliable communication platform. These devices allow users to type out messages, which can be spoken aloud by the device.
- Custom Vocabulary Sets: Customizing the AAC device with vocabulary sets that are meaningful and relevant to the individual’s daily life, activities, and preferences. This ensures the device is user-friendly and encourages active use.
- Ongoing Assessment: Regularly reassessing the individual’s communication needs and abilities to ensure the AAC system remains appropriate and effective. Adjustments and updates should be made as needed to support evolving communication goals.
Comprehensive Management and Care Strategies
- Medical Management:
- Hydrocephalus Control: Surgical implantation of a VP shunt to manage hydrocephalus and relieve intracranial pressure.
- Seizure Management: Antiepileptic medications to control seizures, tailored to the individual’s needs.
- Sleep Management: Addressing sleep disturbances through behavioral interventions and medications as needed.
- Gastrointestinal Care: Managing feeding difficulties and gastrointestinal issues through dietary modifications and, if necessary, feeding tubes.
- Orthopedic Management: Regular monitoring and treatment of orthopedic issues such as scoliosis and hip dislocation by specialists.
- Vision and Hearing: Routine assessments by ophthalmologists and audiologists to address visual and auditory impairments.
- Behavioral and Psychological Support:
- Behavioral Interventions: Utilizing behavioral therapies, including Applied Behavior Analysis (ABA) and behavior modification strategies, to manage hyperactivity, attention deficits, and other behavioral challenges.
- Psychological Support: Providing psychological support for both the individual and their family through counseling and support groups.
- Reinforcement Strategies: Implementing positive reinforcement strategies to encourage desired behaviors and skills.
- Therapies and Interventions:
- Physical Therapy: Focused on improving motor skills, balance, and coordination through regular therapy sessions.
- Occupational Therapy: Assisting with daily living skills, sensory processing, and fine motor skills. Recommending adaptive equipment to support independence.
- Speech and Language Therapy: Essential for developing communication skills, with early introduction of AAC devices and non-verbal communication methods.
- Hydrotherapy: Water-based therapies to improve muscle strength, coordination, and relaxation, making them a beneficial adjunct to traditional therapies.
-
Educational Strategies:
- Specialized Education Plans: Developing individualized education plans (IEPs) that cater to the specific needs of the child. These plans should be flexible and adaptable to the child's evolving capabilities and needs.
- Inclusion Strategies: Including children with Dandy-Walker Syndrome in mainstream classrooms with appropriate supports can enhance social interactions and provide a more inclusive educational experience.
- Use of Technology: Integrating technology in education through tablets, interactive apps, and other digital tools can aid learning and engagement.
-
Family and Community Support:
- Support Groups: Connecting with other families through support groups can provide emotional support, practical advice, and a sense of community.
- Respite Care: Providing families with access to respite care services can offer much-needed breaks, helping to prevent caregiver burnout.
- Advocacy and Resources: Educating families about available resources, advocacy organizations, and legal rights ensures they can access necessary services and support.
Challenges and Considerations
- Medical Challenges: Managing multiple medical issues, including seizures, sleep disturbances, and feeding difficulties, requires a coordinated approach involving various healthcare professionals.
- Educational Barriers: Ensuring that educational strategies are tailored to the child's unique learning needs and that educators are trained to support these needs effectively.
- Behavioral Issues: Addressing behavioral challenges such as hyperactivity and attention deficits through consistent behavioral strategies and therapeutic interventions.
- Social Integration: Promoting social interactions and inclusion within the community to enhance the individual's quality of life and prevent social isolation.
Future Directions and Research
- Genetic Research: Ongoing research into the genetic mechanisms underlying Dandy-Walker Syndrome holds promise for future treatments and potential cures. Gene therapy and other advanced techniques are being explored.
- Clinical Trials: Participation in clinical trials can provide access to new treatments and therapies, contributing to the broader understanding of the syndrome and improving care.
- Therapeutic Innovations: Developing new therapeutic approaches, including targeted medications, advanced AAC technologies, and innovative behavioral interventions, to enhance the quality of life for individuals with Dandy-Walker Syndrome.
References
This section provides key research and clinical resources.
Additional Resources
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Dandy Walker Syndrome?
What does Dandy Walker Syndrome do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.