Introduction
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Infarction
- Pathology: Variable
- Rarity Classification: Ultra-Orphan
- Typical Onset: Any Age
- Gender Impact: Either Gender
- Seizure Prevalence: Variable (Subtype)
- Population Trend: Unknown
Pathophysiology
Ideopathic cerebral lesion growth
AAC Considerations
Recommended Access Modalities: Touch
Additional Clinical Notes
Facial paralysis secondary to poor brain oxygenation secondary to multiple possible pathologies
Quick Reference
| Metric | Value |
|---|---|
| Incidence | Unknown (ultra-rare, <150 cases in literature) |
| Prevalence | Rare (<40 cases from ischemic stroke) |
| Age of Onset | Variable (acquired, typically adult onset) |
| AT Required | Nearly 100% require AAC due to severe dysarthria and dysphagia |
Foix-Chavany-Marie Syndrome
Formal Name: Foix-Chavany-Marie Syndrome (Bilateral Anterior Opercular Syndrome)
Demographic Information
- Incidence: Rare, with fewer than 1,000 cases reported globally.
- Prevalence: Extremely rare, exact prevalence unknown.
- Gender: Affects both males and females equally.
- Onset Age: Can present at any age, from childhood to adulthood.
Coding
- ICD-11: 8A82.1
- ICD-10-CM: G12.29
- OMIM: 304020
- UMLS: C0268463
- MeSH: Not specifically coded
- GARD: 7346
Medical Features and Pathophysiology
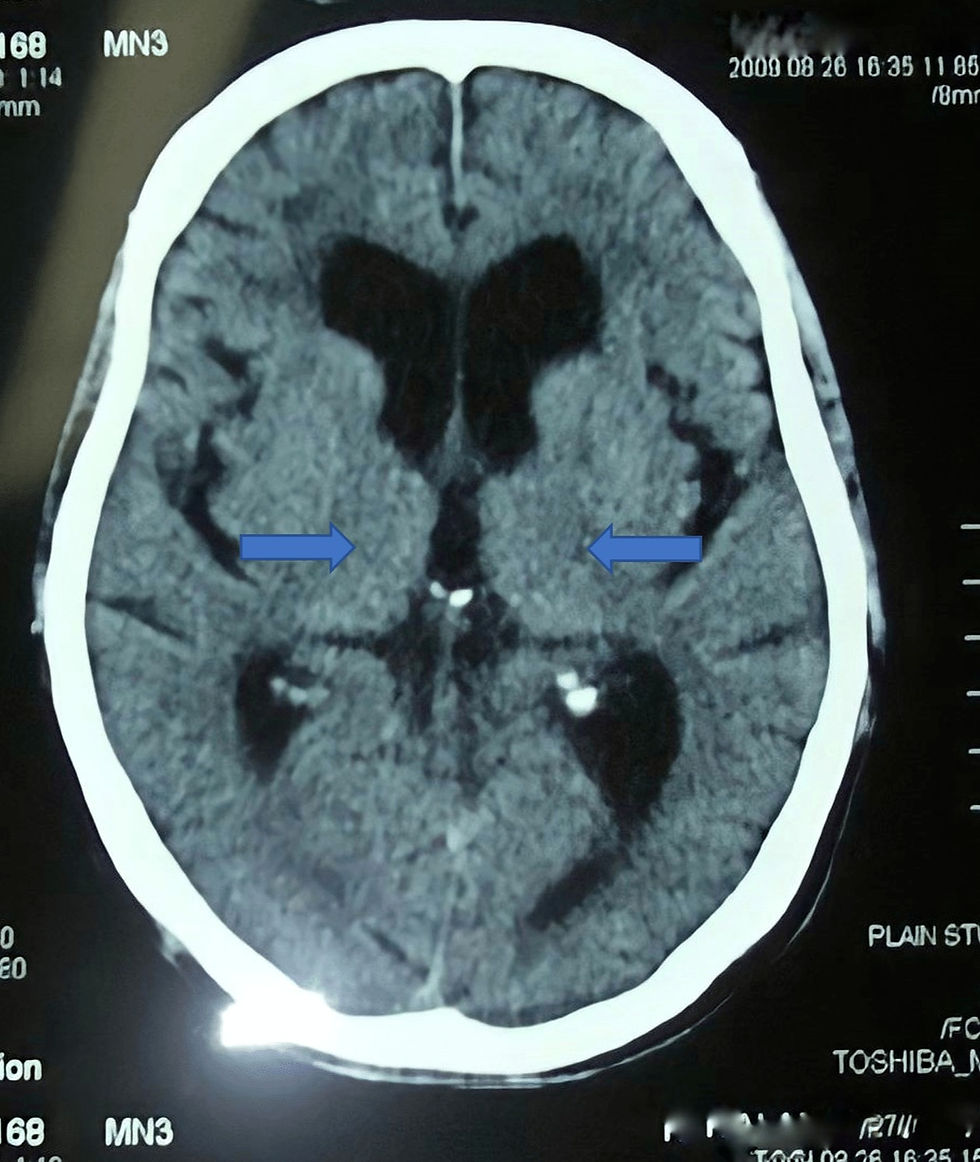
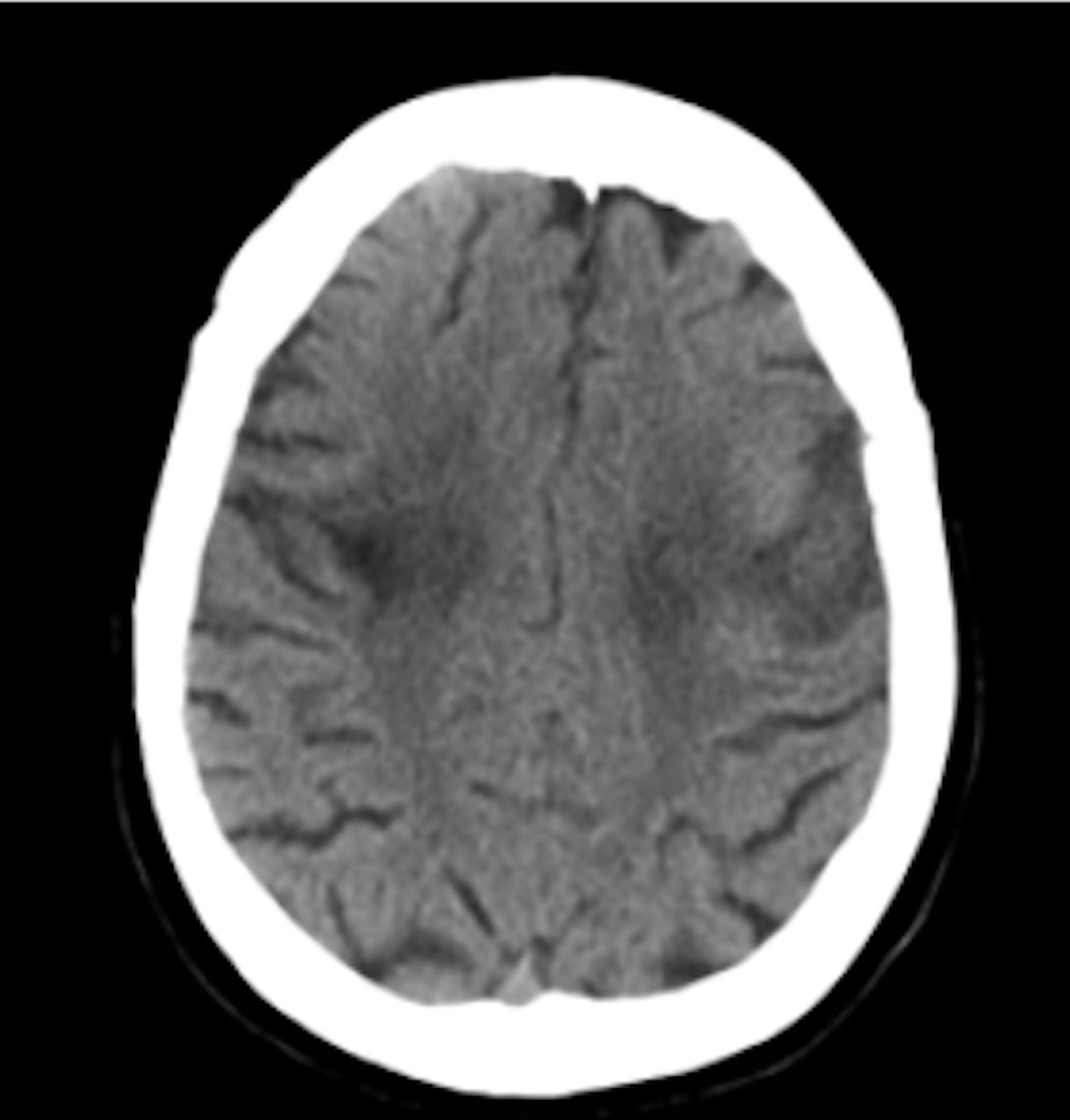
- Etiology: Foix-Chavany-Marie Syndrome (FCMS) is caused by bilateral lesions in the anterior opercular region of the brain. These lesions typically result from strokes, infections, traumatic brain injury, or neurodegenerative diseases. The syndrome is characterized by damage to cranial nerves V (trigeminal), VII (facial), IX (glossopharyngeal), X (vagus), and XII (hypoglossal), which leads to both motor and sensory deficits in the face, pharynx, and jaw.
- Pathology: FCMS presents with severe dysarthria and dysphagia due to the paralysis of masticatory, facial, pharyngeal, and lingual muscles. This paralysis occurs alongside preserved automatic movements such as emotional smiling, laughing, and crying, indicating an automatic-voluntary dissociation. The patients typically have a slack jaw, are unable to voluntarily close their mouths, and display pseudo-peripheral bilateral facial paresis. The syndrome also often includes severe speech impairments, with many patients being anarthric or mute but retaining the ability to communicate through writing or gestures.
- Symptoms:
- Facial and Oral Motor Deficits: Inability to control facial, tongue, pharyngeal, and masticatory muscles voluntarily.
- Speech and Swallowing Impairments: Severe dysarthria, often progressing to complete mutism (anarthria); dysphagia necessitating tube feeding.
- Automatic Movements: Preservation of involuntary movements such as emotional expressions and yawning.
- Additional Symptoms: Sialorrhea (excessive drooling), hyperactive jaw jerk, absent or depressed gag reflex, and potentially severe developmental delays in congenital cases.
- Diagnosis: Diagnosis is primarily clinical, supported by neuroimaging studies such as MRI and CT scans that reveal bilateral lesions in the anterior opercular region. Differential diagnosis includes conditions such as pseudobulbar palsy, bulbar palsy, Guillain-Barré syndrome, myasthenia gravis, and brainstem strokes.
Assistive Suggestions and Requirements
Nearly 100% of individuals with FCMS require AAC due to severe dysarthria or anarthria. The preserved ability to write or gesture in many cases offers critical access pathways. Unlike many neurodegenerative conditions, FCMS often spares limb function, making direct selection via touchscreen or keyboard viable despite complete loss of oral speech.
Assistive Technology Suggestions: - Communication Devices: AAC devices, including picture boards and speech-generating devices. - Feeding Aids: Gastrostomy tubes for severe dysphagia. - Mobility Aids: Customized wheelchairs for individuals with associated motor impairments.
Access Modalities: - Switch Access: Suitable for severe motor impairments. - Eye-Gaze Technology: Enables control through eye movements for severe limb and facial motor deficits. - Touchscreen Devices: Beneficial for individuals retaining hand function.
Care Management and Therapeutic Techniques
- Aims:
- Improve Communication: Enhance communication through AAC devices and tailored speech therapy.
- Ensure Safe Feeding: Manage dysphagia to prevent aspiration and provide adequate nutrition through alternative feeding methods.
- Support Daily Living: Assist with activities of daily living through adaptive equipment and technologies.
- Family and Caregiver Support: Provide education, resources, and emotional support to families.
- SLP Suggestions:
- AAC Implementation: Introduce and regularly update AAC devices to meet the evolving needs of the individual.
- Swallowing Therapy: Implement strategies to improve safe swallowing and reduce the risk of aspiration.
- Communication Training: Educate family members and caregivers on effective communication techniques using AAC devices.
- Special Educator Suggestions:
- Individualized Education Plans (IEP): Develop and adapt IEPs to address the unique learning needs and capabilities of the individual.
- Inclusive Strategies: Use visual supports, structured routines, and differentiated instruction to create an inclusive educational environment.
- Sensory Integration: Incorporate sensory activities to help with sensory processing issues.
- Occupational Therapist Suggestions:
- Adaptive Equipment: Recommend and train the use of adaptive equipment for daily tasks.
- Motor Skill Development: Implement exercises to improve fine and gross motor skills.
- Positioning and Mobility: Ensure proper positioning and support in wheelchairs and other seating systems.
- Recommendations on AAC:
- Symbol-Based Communication: Use symbol-based communication systems for individuals with limited verbal abilities.
- Text-Based Communication: Provide text-based AAC devices for those who can read and write.
- Ongoing Assessment: Regularly reassess communication needs to ensure the AAC system remains effective.
Comprehensive Management and Care Strategies
- Medical Management:
- Seizure Control: Use antiepileptic medications if seizures are present.
- Infection Control: Monitor and treat any infections promptly, especially those affecting the brain.
- Neuroimaging: Regular imaging to monitor the progression of lesions and guide treatment plans.
- Behavioral and Psychological Support:
- Behavioral Interventions: Use behavioral therapies to manage hyperactivity and attention deficits.
- Psychological Support: Provide counseling and support groups for individuals and their families.
- Reinforcement Strategies: Use positive reinforcement to encourage desired behaviors.
- Therapies and Interventions:
- Physical Therapy: Focus on improving motor skills and coordination.
- Occupational Therapy: Assist with daily living skills and sensory processing.
- Speech and Language Therapy: Develop communication skills using AAC and non-verbal methods.
- Educational Strategies:
- Specialized Education Plans: Develop flexible and adaptable education plans.
- Inclusion Strategies: Promote inclusion in mainstream classrooms with appropriate supports.
- Use of Technology: Integrate technology in education to aid learning and engagement.
- Family and Community Support:
- Support Groups: Connect families with support groups for emotional and practical support.
- Respite Care: Provide access to respite care services for caregivers.
- Advocacy and Resources: Educate families about available resources and advocacy organizations.
Future Directions and Research
- Genetic Research: Explore genetic mechanisms underlying FCMS for potential treatments.
- Clinical Trials: Encourage participation in clinical trials to discover new therapies.
- Therapeutic Innovations: Develop new therapeutic approaches to improve quality of life.
References
This section provides key research and clinical resources.
Additional Resources
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Foix Chavany Marie Syndrome?
What does Foix Chavany Marie Syndrome do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.