Introduction

Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Mutation - De Novo
- Rarity Classification: Orphan
- Typical Onset: Birth
- Gender Impact: Either Gender
- Seizure Prevalence: Yes (>90%)
- Population Trend: Unknown
Pathophysiology
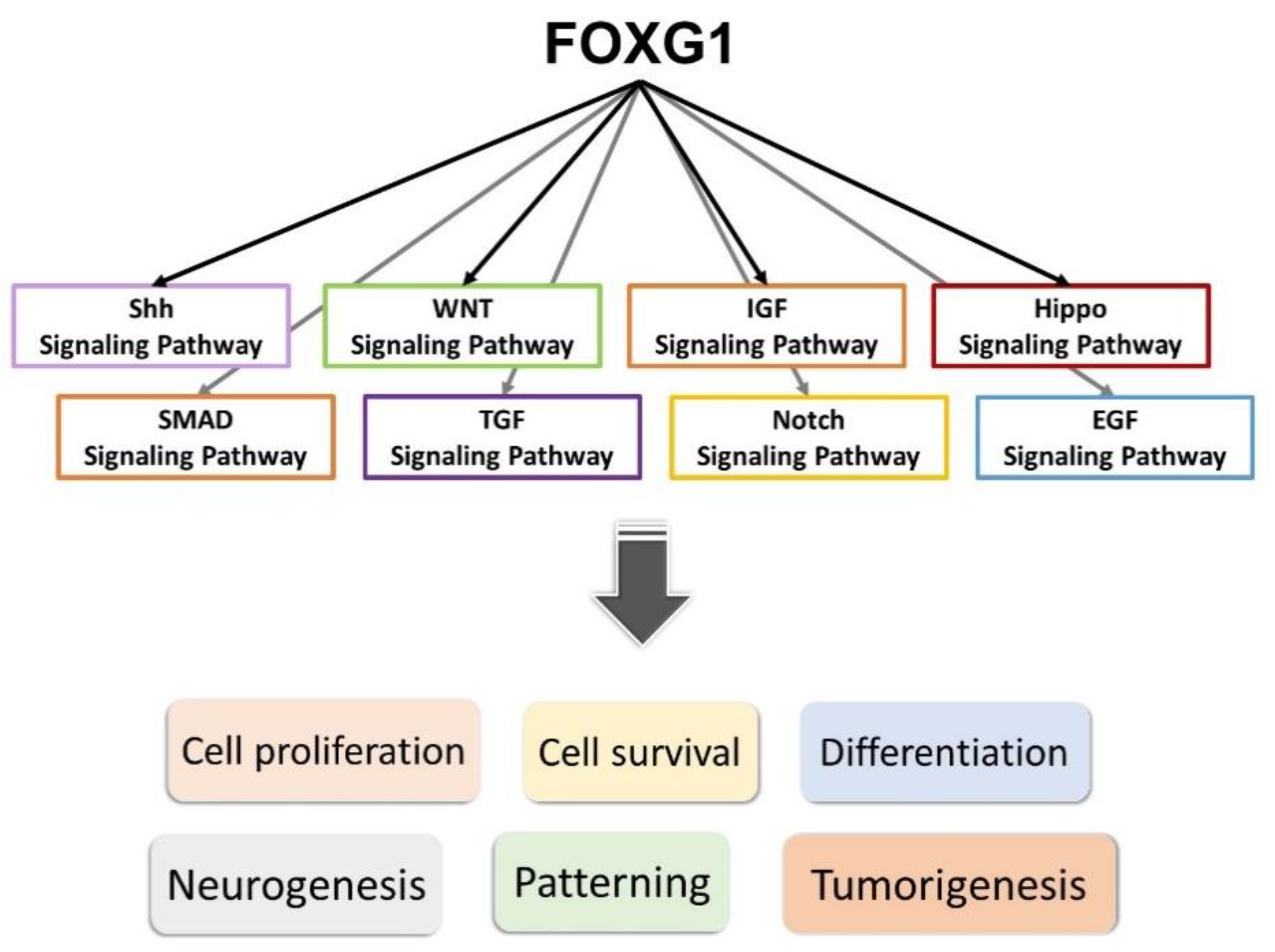
FOXG1 gene (surprise!), either via mutation or deletion of the portion of Chromosome 14 that contains it. Resulting disruption to production of the protein "forkhead box G1" negatively impacts structural development of the brain.
AAC Considerations
Recommended Access Modalities: All - Variable
Additional Clinical Notes
Once called "Congenital Rett;" exceptionally rare but similar presentation that occurs beginning at birth in both genders.
Patient Advocacy & Support Organizations
FOXG1 Syndrome
Name of Disorder: FOXG1 Syndrome
Formal Name: FOXG1 Syndrome
Demographic Information
- Incidence: Not precisely known due to its rarity, but estimated to affect several hundred individuals worldwide.
- Prevalence: Extremely rare, with estimates suggesting a few hundred diagnosed cases globally.
- Gender: Affects both males and females equally.
- Onset Age: Symptoms generally become noticeable within the first year of life, often as early as the second month.
Coding
- ICD-11: 8A04.22
- ICD-10-CM: Q87.89
- OMIM: 164874
- UMLS: C4011086
- MeSH: Not specifically listed
- GARD: 003311
Medical Features and Pathophysiology
- Etiology: FOXG1 Syndrome is caused by mutations in the FOXG1 gene located on chromosome 14. This gene is critical for brain development, and mutations can include deletions, duplications, or missense mutations that affect gene function. These mutations typically occur de novo, meaning they are new mutations in the affected individual and not inherited from the parents.
- Pathology: FOXG1 Syndrome is characterized by impaired development and structural brain abnormalities. Key features include microcephaly (small head size), agenesis of the corpus callosum (absence of the brain structure connecting the two hemispheres), and reduced folds on the surface of the brain. Neurological features often include epilepsy, cortical visual impairment, and severe developmental delays affecting both motor and cognitive functions.
- Symptoms:
- Neurological Symptoms: Frequent seizures, often difficult to control with medication; movement disorders such as involuntary movements and spasticity; cortical visual impairment; and severe intellectual disability.
- Developmental Symptoms: Delayed development of gross and fine motor skills, often resulting in difficulty or inability to sit, walk, or use hands purposefully; significant speech and language delays or disabilities; and challenges with daily living skills such as eating, dressing, and toilet training.
- Behavioral and Physical Symptoms: Repetitive or stereotypical behaviors, irritability and excessive crying, sleep disturbances, scoliosis, strabismus (crossed eyes), and feeding difficulties including gastroesophageal reflux and constipation.
- Diagnosis: Diagnosis typically involves a combination of clinical evaluation and genetic testing. Genetic sequencing tests are essential to confirm mutations in the FOXG1 gene. MRI scans of the brain are also important to identify characteristic structural abnormalities.
Assistive Suggestions and Requirements
Nearly all individuals with FOXG1 Syndrome require assistive technology due to profound cognitive and motor impairments. Communication development is severely limited, with most individuals remaining nonverbal. Cortical visual impairment may affect candidacy for eye-gaze systems, requiring careful assessment of visual function before implementation.
Assistive Technology Suggestions: - Communication Devices: AAC devices, such as speech-generating devices and communication boards. - Mobility Aids: Customized wheelchairs and mobility aids for balance and coordination issues. - Educational Tools: Tablets with specialized apps for cognitive development. - Environmental Control Systems: Systems enabling environmental control using adaptive switches.
Access Modalities: - Switch Access: For individuals with limited motor skills. - Eye-Gaze Technology: May be limited by cortical visual impairment; requires thorough assessment. - Touchscreen Devices: Beneficial for individuals with functional hand use, though cognitive limitations may restrict complexity.


Care Management and Therapeutic Techniques
- Aims:
- Seizure Management: Effective management to reduce frequency and severity through appropriate medications and interventions.
- Developmental Support: Maximizing developmental potential through early and ongoing interventions focusing on cognitive, motor, and communication skills.
- Daily Living Assistance: Providing support for activities of daily living to enhance independence and quality of life through assistive technologies and adaptive equipment.
- Family Support: Offering education, resources, and emotional support to families to help them navigate the challenges associated with FOXG1 Syndrome.
- SLP Suggestions:
- Early Intervention: Speech and language therapy initiated as early as possible to support communication skills.
- AAC Implementation: Introducing AAC devices tailored to individual needs, with regular updates to keep the vocabulary relevant.
- Oral Motor Therapy: Addressing feeding and swallowing difficulties through targeted exercises and strategies.
- Family Training: Educating family members on using AAC devices and communication strategies consistently at home.
- Special Educator Suggestions:
- Individualized Education Plan (IEP): Developing and regularly updating an IEP tailored to the student's strengths and needs.
- Sensory Integration Therapy: Incorporating sensory activities to help with sensory processing issues, improving focus and engagement.
- Inclusive Classroom Strategies: Utilizing visual supports, structured routines, and differentiated instruction to create an inclusive learning environment.
- Life Skills Training: Emphasizing the development of life skills to promote independence in daily living activities.
- Occupational Therapist Suggestions:
- Motor Skill Development: Implementing exercises to improve fine and gross motor skills.
- Adaptive Equipment: Recommending and training the use of adaptive equipment for daily tasks.
- Sensory Processing: Addressing sensory processing issues through tailored sensory diets and activities.
- Positioning and Mobility: Ensuring proper positioning and support in wheelchairs and other seating systems.
- Recommendations on AAC:
- Symbol-Based Communication: Using symbol-based systems for individuals with limited verbal abilities.
- Text-Based Communication: For those who can read and write, text-based AAC devices can provide a reliable communication platform.
- Custom Vocabulary Sets: Customizing AAC devices with vocabulary sets relevant to the individual's daily life and preferences.
- Ongoing Assessment: Regularly reassessing communication needs to ensure the AAC system remains appropriate and effective.
Comprehensive Management and Care Strategies
- Medical Management:
- Seizure Control: Use of antiepileptic medications to manage seizures, potentially including newer medications being studied.
- Sleep Management: Behavioral interventions and medications like melatonin to improve sleep patterns.
- Gastrointestinal Care: High-calorie formulas or gastrostomy tube feeding for severe feeding problems.
- Orthopedic Management: Monitoring and treating orthopedic issues like scoliosis through physical therapy and orthopedic specialist assessments.
- Vision and Hearing: Regular assessments to address visual or auditory impairments.
- Behavioral and Psychological Support:
- Behavioral Interventions: Behavioral therapies such as Applied Behavior Analysis (ABA) to manage hyperactivity and attention deficits.
- Psychological Support: Providing counseling and support groups for both individuals and families.
- Reinforcement Strategies: Using positive reinforcement to encourage desired behaviors and skills.
- Therapies and Interventions:
- Physical Therapy: Improving motor skills, balance, and coordination.
- Occupational Therapy: Assisting with daily living skills and sensory processing.
- Speech and Language Therapy: Developing communication skills through AAC and other methods.
- Hydrotherapy: Water-based therapies to improve muscle strength and relaxation.
- Educational Strategies:
- Specialized Education Plans: Individualized plans catering to specific learning needs.
- Inclusion Strategies: Including children in mainstream classrooms with appropriate supports.
- Use of Technology: Integrating technology in education through tablets and interactive apps.
- Family and Community Support:
- Support Groups: Connecting families through support groups.
- Respite Care: Providing access to respite care services.
- Advocacy and Resources: Educating families about available resources and legal rights.
Challenges and Considerations
- Medical Challenges: Coordinating care across multiple medical issues.
- Educational Barriers: Ensuring educational strategies are tailored to the child's needs.
- Behavioral Issues: Consistent behavioral strategies to address challenges.
- Social Integration: Promoting inclusion and social interactions.
Future Directions and Research
- Genetic Research: Ongoing research into genetic mechanisms and potential treatments.
- Clinical Trials: Participation in trials for new treatments.
- Therapeutic Innovations: Developing new therapeutic approaches to enhance quality of life.
Conclusion
FOXG1 Syndrome is a rare and severe neurodevelopmental disorder presenting significant challenges for individuals, families, and healthcare professionals. While no cure currently exists, a multidisciplinary approach incorporating assistive technology, speech and language therapy, and supportive interventions can maximize potential, improve quality of life, and support the highest achievable level of independence. Ongoing research offers hope for more effective treatments.
References
This section provides key research and clinical resources.
Additional Resources
-
, et al. (2008). FOXG1 Is Responsible for the Congenital Variant of Rett Syndrome. The American Journal of Human Genetics. https://doi.org/10.1016/j.ajhg.2008.05.015 Link [PDF]
-
, et al. (2008). FOXG1 Is Responsible for the Congenital Variant of Rett Syndrome. The American Journal of Human Genetics. https://doi.org/10.1016/j.ajhg.2008.05.015 Link [PDF]
Epidemiology and Demographics
Etiology and Pathophysiology
What causes FOXG1 Syndrome?
What does FOXG1 Syndrome do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.