Introduction
Friedreich's Ataxia (FA) is a rare genetic disorder affecting approximately 1 in 50,000 individuals worldwide. It's caused by mutations in the FXN gene, leading to a deficiency in the frataxin protein, which results in cellular damage, particularly in nerve and muscle cells. Symptoms include progressive gait and limb ataxia, muscle weakness, cardiac issues, and diabetes mellitus. Diagnosis involves clinical examination, genetic testing, and additional tests. Most individuals with FA will require assistive technology due to progressive physical and neurological impairments. Management strategies include symptom management, multidisciplinary approach, speech therapy, individualized education plans, and occupational therapy. Medical management, behavioral and psychological support, early intervention programs, and educational strategies are also crucial. Ongoing studies into the genetic mechanisms of FA and potential gene therapies are future research directions.

Friedreich's Ataxia
Formal Name: Friedreich's Ataxia (FA)
Demographic Information
- Incidence: Approximately 1 in 50,000 individuals worldwide
- Prevalence: Most common hereditary ataxia, especially in people of European descent
- Gender: Affects both males and females equally
- Onset Age: Typically between 5 and 15 years, but can range from early childhood to adulthood
Coding
- ICD-11: 8C72.1
- ICD-10-CM: G11.11
- OMIM: 229300 - Friedreich's Ataxia
- UMLS: C0016733 - Friedreich's Ataxia
- MeSH: D020967 - Friedreich's Ataxia
- GARD: 11654 - Friedreich's Ataxia
Quick Reference
| Quick Facts | Details |
|---|---|
| Incidence | Approximately 1.5 per 100,000 per year (global: 1 in 22,000 to 1 in 50,000) |
| Prevalence | Approximately 1 in 40,000-50,000 in the U.S. (~4,000 patients); most common hereditary ataxia (~50% of all ataxia cases) |
| Gender Distribution | Affects both males and females equally (autosomal recessive inheritance) |
| Primary Age of Onset | Typically between 5-15 years; mean onset 10.5 years; almost always before age 20 |
| AT/AAC Requirements | High - Progressive condition; 75-90% will require assistive technology; AAC challenged by upper limb ataxia and visual disturbances; communication needs increase with disease progression |
Medical Features and Pathophysiology
- Etiology: Friedreich's Ataxia is caused by mutations in the FXN gene on chromosome 9, which leads to a deficiency in the frataxin protein. This protein is crucial for mitochondrial function, and its deficiency results in the accumulation of iron in the mitochondria, causing oxidative stress and cellular damage, particularly in nerve and muscle cells.
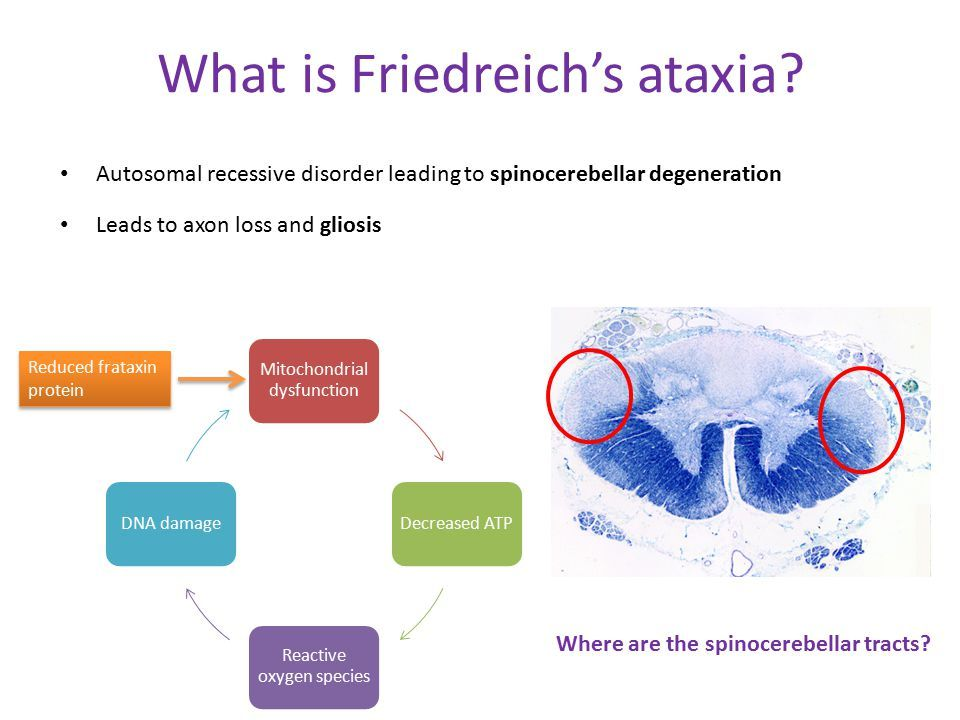
- Pathology: The disease primarily affects the spinal cord, peripheral nerves, and the cerebellum, leading to progressive damage. The heart and pancreas can also be affected, resulting in cardiomyopathy and diabetes mellitus.
- Symptoms:
- Neurological: Progressive gait and limb ataxia, dysarthria (slurred speech), dysphagia (difficulty swallowing), loss of deep tendon reflexes, and loss of proprioception (sense of body position).
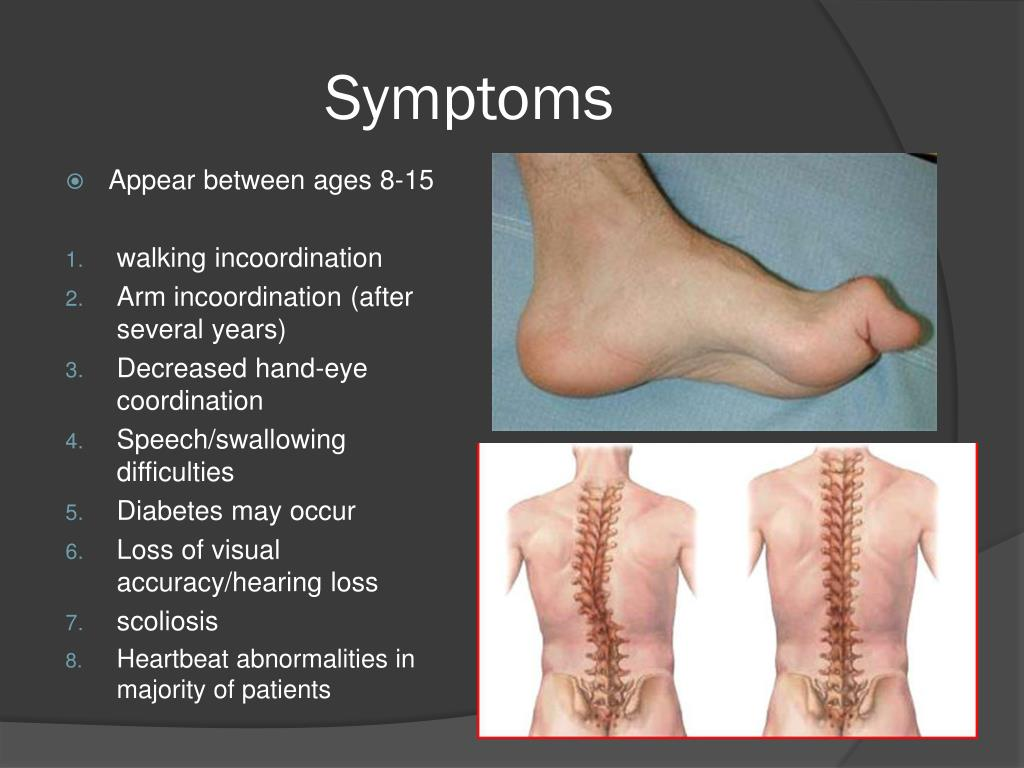
- Musculoskeletal: Muscle weakness and atrophy, scoliosis (curvature of the spine), and foot deformities such as pes cavus (high arches).
- Cardiac: Hypertrophic cardiomyopathy, arrhythmias, and heart failure.
- Endocrine: Diabetes mellitus.
- Sensory: Vision and hearing loss can occur in the later stages.
- Diagnosis: Diagnosis involves a combination of clinical examination, genetic testing to identify FXN gene mutations, and additional tests such as MRI or CT scans, electromyograms (EMG), nerve conduction studies, echocardiograms, and blood tests to evaluate glucose and vitamin E levels.
Assistive Suggestions and Requirements
- Requirement Percentage for Assistive Technology: Approximately 75-90% of individuals with Friedreich's Ataxia will require assistive technology at some point due to progressive physical and neurological impairments.
- Assistive Technology Suggestions:
- Mobility Aids: Customized wheelchairs, walkers, and braces to support mobility and posture.
- Communication Devices: AAC devices to assist with speech difficulties.
- Environmental Control Systems: Systems that allow control of home devices to enhance independence.
- Access Modalities:
- Switch Access: Suitable for those with severe motor impairments.
- Voice Activation: For individuals who retain adequate speech abilities.
- Eye-Gaze Technology: For those with significant motor impairments affecting hand use.
Care Management and Therapeutic Techniques
- Aims:
- Symptom Management: Alleviating symptoms and maintaining function and quality of life.
- Multidisciplinary Approach: Coordination among neurologists, cardiologists, endocrinologists, physical therapists, and speech therapists.
- SLP Suggestions:
- Speech Therapy: To address dysarthria and dysphagia, focusing on articulation, breathing techniques, and safe swallowing strategies.
- AAC Implementation: Introducing and training in the use of AAC devices for effective communication.
- Special Educator Suggestions:
- Individualized Education Plan (IEP): Developing an IEP that includes accommodations for physical and learning disabilities.
- Assistive Technology: Using technology to facilitate learning and participation in educational activities.
- Life Skills Training: Emphasizing the development of independent living skills.
- Occupational Therapist Suggestions:
- Fine Motor Skills: Exercises to maintain dexterity and coordination.
- Adaptive Equipment: Recommendations for utensils, writing aids, and dressing tools to enhance daily living activities.
- Sensory Integration: Techniques to manage sensory processing issues.
- Recommendations on AAC:
- Symbol-Based Communication: For those with severe speech impairments.
- Text-Based Communication: For individuals who can read and write.
- Customized Vocabulary Sets: Tailoring AAC devices to include relevant vocabulary and phrases.
- Ongoing Assessment: Regularly reassessing communication needs and updating AAC systems accordingly.
Comprehensive Management and Care Strategies
- Medical Management:
- Medication: Managing symptoms such as heart issues and diabetes with appropriate medications. The FDA-approved medication omaveloxolone may be used in individuals 16 years and older.
- Therapies: Physical, occupational, and speech therapies to maintain function and address symptoms.
- Monitoring: Regular cardiological and neurological evaluations to manage disease progression.
- Behavioral and Psychological Support:
- Counseling: Providing psychological support to patients and caregivers to cope with the emotional and mental health challenges.
- Support Groups: Facilitating connections with other families and individuals affected by FA.
- Therapies and Interventions:
- Early Intervention Programs: Initiating therapies early to maximize developmental outcomes.
- Educational Support: Adapting educational strategies to accommodate physical and cognitive limitations.
- Physical and Occupational Therapies: Focused on maintaining mobility, strength, and daily living skills.
- Educational Strategies:
- Inclusive Education: Strategies to integrate students with FA into mainstream classrooms with appropriate supports.
- Technology Integration: Utilizing assistive technology to enhance learning and participation.
- Family and Community Support:
- Respite Care: Providing temporary relief for primary caregivers to prevent burnout.
- Advocacy and Resources: Educating families about available resources and support systems.
Challenges and Considerations
- Medical Challenges: Managing multiple health issues, including cardiac and endocrine complications.
- Educational Barriers: Ensuring educational strategies are tailored to individual needs.
- Behavioral Issues: Addressing behavioral challenges through consistent strategies and interventions.
- Social Integration: Promoting social interactions and community participation to improve quality of life.
Future Directions and Research
- Genetic Research: Ongoing studies into the genetic mechanisms of FA and potential gene therapies.
- Clinical Trials: Participation in trials for new treatments and interventions.
- Therapeutic Innovations: Developing new therapies to improve quality of life for individuals with FA.
Demographics
- Incidence: Estimated at 1 in 50,000 individuals worldwide.
- Prevalence: Approximately 1 in 29,000 individuals in the United States.
- Gender Distribution: Affects both males and females equally.
- Typical Age of Onset: Symptoms typically appear between ages 5 and 15.
Coding
- ICD-11: 8C72.0
- OMIM: 229300
- UMLS: C0002736
- MeSH: D005600
- GARD: 0007324
Overview
Friedreich's Ataxia (FA) is a rare, inherited disorder that causes progressive damage to the nervous system, leading to movement and sensory symptoms, walking difficulties, and impaired balance. It is the most common form of hereditary ataxia in the United States.
Key Features
- Movement and Sensory Symptoms: Awkward movements, impaired muscle coordination, difficulty walking, sensory loss, slurred speech, muscle tone changes, scoliosis, swallowing difficulties, and fatigue.
- Progression: Symptoms typically start between ages 5-15, with individuals possibly needing a wheelchair within 10-20 years. Heart disease and diabetes are common complications.
Medical Features and Pathophysiology
Pathophysiology
- Genetic Basis: FA is caused by a mutation in the FXN gene, leading to abnormal frataxin production, which affects mitochondrial function.
- Autosomal Recessive Inheritance: Individuals need two defective copies of the FXN gene to develop FA.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Heritable
- Rarity Classification: Orphan
- Typical Onset: Childhood
- Gender Impact: Either Gender
- Progressive/Degenerative: Yes
- Seizure Prevalence: No (<10%)
- Population Trend: Stable
Pathophysiology
FXN gene abnormality (mitochondrial dna) causing a GAA trinucleotide repeat; that genetic tract expansion is more likely to manifest ataxia with a higher number of repeats, just as in Huntingtons and related disorders.
AAC Considerations
Recommended Access Modalities: All - Progression
Additional Clinical Notes
Neurodegenerative disorder with onset of 10-15 years; structural abnormalities in the feet can be an early giveaway. one of many conditions implicating the FXN gene, and may be underdiagnosed
Patient Advocacy & Support Organizations
- http://curefa.org/whatis
- https://friedreichsataxianews.com/2017/08/07/five-symptoms-of-freidreich-ataxia/
Symptoms
Early Signs (Childhood):
- Difficulty walking and poor balance.
- Slurred speech and difficulty swallowing.
- Loss of sensation in the arms and legs.
- Muscle weakness and fatigue.
Later Symptoms (Adolescence and Adulthood):
- Progressive loss of coordination and muscle strength.
- Scoliosis (curvature of the spine).
- Heart disease, including hypertrophic cardiomyopathy.
- Diabetes mellitus.
- Hearing and vision loss.
Diagnosis
- Genetic Testing: DNA testing to identify mutations in the FXN gene, which confirms the diagnosis of FA.
- Clinical Evaluation: A thorough medical history, physical examination, and neurological assessment to identify characteristic features of FA.
- Neuroimaging: Magnetic Resonance Imaging (MRI) of the brain and spinal cord to assess structural abnormalities.
- Electromyography (EMG) and Nerve Conduction Studies: To evaluate the electrical activity of muscles and the speed of nerve signals.
- Cardiac Evaluation: Electrocardiogram (EKG) and echocardiogram to assess heart function.
- Glucose Tolerance Test: To check for diabetes mellitus.
Management and Treatment
There is no cure for FA, and treatment focuses on managing symptoms and supporting development.
Medications
- Antioxidants: To reduce oxidative stress and protect nerve cells. Examples include idebenone and coenzyme Q10.
- Heart Medications: To manage heart disease, including beta-blockers and ACE inhibitors.
- Diabetes Medications: To control blood sugar levels in individuals with diabetes mellitus.
Therapies
- Physical Therapy: To improve muscle strength, coordination, balance, and mobility.
- Occupational Therapy: To develop fine motor skills, adaptive skills for daily living, and sensory processing.
- Speech and Language Therapy: To address communication challenges and improve speech clarity and swallowing function.
- Behavioral Therapy: To address challenging behaviors, promote positive behaviors, and teach coping mechanisms.
- Educational Support: Individualized Education Plans (IEPs) to provide tailored educational services and support.
Assistive Technology and Communication Devices
Assistive technology plays a crucial role in enhancing communication, independence, and quality of life for individuals with FA. Given the speech and language difficulties and motor impairments associated with FA, many individuals may benefit from assistive technology.
Speech Generating Devices (SGDs)
Individuals with FA often have significant speech and language impairments. Augmentative and Alternative Communication (AAC) is crucial for enabling them to express their needs, thoughts, and feelings.
Importance of Symbols for Individuals with FA
Visual symbols support communication for individuals with Friedreich's Ataxia by leveraging visual processing strengths and providing concrete representations of language concepts.
Symbol selection should be individualized based on visual skills, motor abilities, and symbolic understanding. Consider using Picture Communication Symbols (PCS), SymbolStix, photographs, or tactile symbols depending on the individual's needs.
Access Methods
The choice of access method is crucial for successful AAC use and depends on an individual's motor, cognitive, and sensory abilities. For individuals with FA, common access methods include:
Direct Selection
Individuals with sufficient motor control may be able to directly select symbols on a screen or communication board using their finger, hand, or a pointer. Key considerations for direct selection with FA include:
- Accuracy: Assess an individual's ability to isolate a finger or accurately use a pointer to select symbols. Larger symbols and increased spacing between symbols may be necessary to accommodate motor challenges.
- Fatigue: Direct selection can be physically taxing, especially for individuals with significant motor impairments. Frequent breaks and careful positioning are essential.
- Interference from Involuntary Movements: Involuntary movements, such as tremors or spasms, can make direct selection challenging. Stabilizing techniques, such as using a keyguard or mounting the device, can help.
Eye Gaze
For individuals with significant motor impairments but good ocular control, eye gaze systems can provide an efficient access method. Key considerations for eye gaze with FA include:
- Calibration: Accurate calibration is essential for successful eye gaze use. This can be challenging for individuals with nystagmus, strabismus, or significant head movements. Multiple calibration attempts or customized calibration settings may be necessary.
- Visual Skills: Assess an individual's visual acuity, visual field, and oculomotor control to determine the appropriateness of eye gaze. Larger symbols, increased spacing, and high-contrast displays may be necessary to accommodate visual impairments.
- Positioning: Proper positioning of both the individual and the eye gaze device is crucial for comfort and accuracy. A stable head position and minimized glare on the screen are important considerations.
Switch Scanning
For individuals with severe motor impairments who cannot reliably point or use eye gaze, scanning allows them to select symbols using a switch or switches. Key considerations for scanning with FA include:
- Cognitive Demands: Scanning requires significant cognitive skills, including attention, timing, and sequencing. Careful assessment of an individual's cognitive profile is essential to determine the appropriateness of scanning.
- Auditory and Visual Prompts: Scanning relies on auditory and/or visual prompts to guide an
Switch Scanning
For individuals with severe motor impairments who cannot reliably point or use eye gaze, scanning allows them to select symbols using a switch or switches. Key considerations for scanning with FA include:
- Cognitive Demands: Scanning requires significant cognitive skills, including attention, timing, and sequencing. Careful assessment of an individual's cognitive profile is essential to determine the appropriateness of scanning.
- Auditory and Visual Prompts: Scanning relies on auditory and/or visual prompts to guide an individual through the selection process. Ensure that the prompts are appropriate given an individual's sensory abilities and preferences.
- Customization: Scanning patterns, speed, and switch placement should be customized to an individual's unique needs and abilities. Ongoing adjustments may be necessary as skills develop or change over time.
- Partner-Assisted Scanning: For individuals with the most severe motor and cognitive impairments, partner-assisted scanning may be the most appropriate access method. In this approach, a communication partner presents choices auditorily or visually, and the individual indicates a choice through a predetermined signal, such as an eye blink or vocalization.
Ultimately, the selection of an access method should be driven by a comprehensive assessment of an individual's strengths, needs, and preferences. Many individuals with FA may benefit from a combination of access methods depending on the context and their changing abilities over time.
Literacy Considerations
While many individuals with FA may not develop traditional literacy skills, it is essential to provide opportunities for literacy development within their AAC systems:
- Exposure to Print: Consistently pairing symbols with printed words can help build print awareness and recognition over time. Even if an individual does not develop independent reading skills, exposure to print can support language development and provide a foundation for future literacy learning.
- Sight Words: Some individuals with FA may develop sight word recognition, even if they do not develop full reading skills. Incorporating personally meaningful sight words into an AAC system can enhance communication efficiency and support participation in literacy-based activities.
- Phonological Awareness: Incorporating activities targeting phonological awareness, such as rhyming or initial sound identification, can lay the groundwork for literacy development. These activities can be adapted to an individual's cognitive and linguistic level and integrated into AAC use.
- Shared Reading: Regularly engaging in shared reading activities, using adapted books with symbol support, can build language skills and foster a love of literacy. Interactive reading techniques, such as pausing for participation or asking questions, can further enhance engagement and comprehension.
Ultimately, literacy goals for individuals with FA should be individualized based on their unique profiles and learning trajectories. AAC systems should be designed to grow with an individual's developing skills and provide ongoing opportunities for literacy learning.
Customization and Implementation
- Personalized Vocabulary Selection: Choose vocabulary that is meaningful and relevant to the individual's daily life, interests, and communication needs.
- Consistency Across Environments: Use the same AAC system and vocabulary at home, school, and in the community to promote generalization and consistent communication.
- Training Communication Partners: Train family members, caregivers, educators, and therapists on how to use the AAC system effectively and support the individual's communication.
Behavioral Considerations
- Attention Span: Individuals with FA often have short attention spans, so AAC interventions should be brief, engaging, and incorporate frequent breaks.
- Hyperactivity: Manage hyperactivity through behavioral strategies, such as providing opportunities for movement and sensory input.
- Motivation: Use motivating activities and reinforcers to encourage active participation in AAC interventions.
Considerations for Visual Impairment
- Tactile Symbols: For individuals with visual impairments, tactile symbols can be used to represent words or concepts.
- Auditory Scanning: AAC devices with auditory scanning capabilities allow individuals to hear options and select them using a switch.
- Enlarged Displays: AAC devices with larger displays or adjustable font sizes can improve visibility for individuals with low vision.
Care Management and Therapeutic Techniques
Aims
- Maximize Potential: Provide opportunities for individuals with FA to develop their skills and abilities to the fullest extent possible.
- Manage Challenges: Address the unique challenges associated with FA, such as movement difficulties, sensory impairments, and speech issues.
- Enhance Communication: Facilitate effective communication using AAC devices, sign language, or other alternative methods.
- Promote Independence: Encourage independence in daily living skills, self-care, and social interactions.
Medical Management
- Regular Medical Check-Ups: Monitor overall health, manage any associated medical conditions, and ensure appropriate growth and development.
- Treatment of Associated Medical Conditions: Address any co-occurring medical conditions, such as heart disease, diabetes, or scoliosis.
- Behavioral and Mental Health Support: Regular monitoring and management of behavioral and mental health issues, including anxiety, depression, and mood disorders.
Therapies and Interventions
- Speech and Language Therapy: Focus on alternative communication methods, such as sign language or AAC devices, and develop speech and language skills.
- Occupational Therapy: Focus on developing fine motor skills, adaptive skills for daily living, and sensory processing.
- Physical Therapy: Focus on improving muscle strength, coordination, balance, and mobility.
- Behavioral Therapy: Focus on addressing challenging behaviors, promoting positive behaviors, and teaching coping mechanisms.
- Music Therapy: Use music to engage individuals with FA, promote communication, and reduce anxiety.
Speech-Language Pathologist (SLP) Suggestions
- Comprehensive Speech and Language Assessment: Conduct a thorough evaluation of the individual's receptive and expressive language abilities, oral-motor skills, and overall communication needs. This assessment should include standardized tests, parent/caregiver interviews, and naturalistic observations.
- Early Intervention: Initiate speech and language therapy as early as possible to maximize communication potential. Focus on developing pre-linguistic skills, such as joint attention, turn-taking, and symbolic play, which lay the foundation for later language development.
- Multimodal Communication Approach: Implement a total communication approach that incorporates various modalities, such as vocalizations, gestures, manual signs, and AAC devices. This approach ensures that the individual always has a means to communicate, even if one modality is temporarily unavailable or ineffective.
- AAC System Selection and Implementation: Work closely with the individual, family, and other professionals to select the most appropriate AAC system based on the individual's abilities, needs, and preferences. Provide ongoing training and support to ensure successful implementation and generalization of AAC use across settings.
- Oral-Motor and Feeding Therapy: Address any oral-motor deficits that may impact speech production, feeding, and swallowing. Implement exercises and strategies to improve muscle strength, coordination, and range of motion in the oral-facial region. Collaborate with occupational therapists and other professionals to manage feeding difficulties and ensure safe swallowing.
- Language Stimulation Techniques: Use evidence-based language stimulation techniques, such as expansions, extensions, and recasts, to promote language growth. Create language-rich environments that encourage communication and provide ample opportunities for the individual to express themselves.
- Social Communication Interventions: Target social communication skills, such as initiating and maintaining interactions, responding to others, and engaging in turn-taking. Use social stories, role-play, and video modeling to teach social norms and expectations.
- Literacy Development: Support emergent literacy skills by incorporating shared book reading, print awareness activities, and phonological awareness tasks into therapy sessions. Adapt literacy materials to accommodate the individual's visual and motor impairments.
- Collaboration and Consultation: Work closely with families, educators, and other professionals to ensure consistent implementation of communication strategies across environments. Provide training and support to caregivers to promote effective communication at home and in the community.
Occupational Therapist Suggestions
- Comprehensive Occupational Therapy Assessment: Conduct a thorough evaluation of the individual's fine motor skills, visual-motor coordination, sensory processing, and adaptive behavior. Use standardized assessments, clinical observations, and parent/caregiver interviews to gather information.
- Fine Motor Skill Development: Implement activities and exercises to improve hand strength, dexterity, and manipulation skills. Use adaptive tools and techniques to accommodate motor impairments and maximize independence in daily tasks.
- Visual-Motor Integration: Address deficits in visual-motor coordination through activities that involve eye-hand coordination, visual tracking, and visual scanning. Use visual cues and tactile feedback to support accurate motor responses.
- Sensory Processing Interventions: Identify sensory processing difficulties and develop individualized sensory diets to help regulate sensory input. Incorporate sensory-based activities, such as deep pressure, weighted vests, and tactile stimulation, into daily routines to promote best arousal and engagement.
- Adaptive Equipment and Environmental Modifications: Recommend and train the individual and caregivers in the use of adaptive equipment, such as special seating systems, mobility devices, and feeding aids. Modify the environment to enhance accessibility, safety, and independence.
- Activities of Daily Living (ADLs): Teach strategies and techniques to improve independence in self-care tasks, such as dressing, grooming, and toileting. Break down complex tasks into smaller steps and use visual supports to facilitate learning.
- Play and Leisure Skills: Promote engagement in age-appropriate play and leisure activities to support cognitive, social, and emotional development. Adapt toys and games to accommodate motor and sensory impairments.
- Collaboration with Other Professionals: Work closely with physical therapists, speech-language pathologists, and educators to ensure a comprehensive and coordinated approach to intervention. Share information and strategies to support the individual's participation and progress across settings.
BCBA/ABA Practitioner Suggestions
- Functional Behavior Assessment (FBA): Conduct comprehensive FBAs to identify the underlying causes of challenging behaviors often associated with FA, such as self-inj
urious behaviors, aggression, or stereotypy. Use this information to develop targeted intervention strategies.
- Individualized Behavior Intervention Plans: Create tailored behavior intervention plans that address specific challenging behaviors while promoting adaptive skills. Focus on positive reinforcement strategies and environmental modifications to support desired behaviors.
- Adaptive Skill Training: Implement programs to develop essential adaptive skills, including toileting, feeding, and basic self-care. Use task analysis and chaining techniques to break down complex skills into manageable steps.
- Social Skills Development: Design interventions to enhance social interaction skills, focusing on nonverbal communication, turn-taking, and appropriate social responses. Utilize social stories and video modeling to support skill acquisition.
- Sensory-Based Interventions: Collaborate with occupational therapists to incorporate sensory integration techniques into behavior interventions, addressing sensory sensitivities or seeking behaviors often observed in individuals with FA.
- Parent and Caregiver Training: Provide extensive training to parents and caregivers on implementing behavior strategies consistently across environments. Emphasize the importance of reinforcement systems and environmental modifications.
- Data-Driven Decision Making: Implement reliable data collection systems to monitor progress and make informed decisions about intervention effectiveness. Regularly analyze data to adjust interventions as needed.
- Collaboration with Medical Team: Work closely with the individual's medical team to understand how medical factors, such as medications, may impact behavior and learning. Adjust interventions accordingly.
Physical Therapist Suggestions
- Comprehensive Physical Therapy Assessment: Conduct a thorough evaluation of the individual's gross motor skills, mobility, balance, and posture. Assess muscle tone, range of motion, and strength to identify areas of concern and guide treatment planning.
- Gross Motor Skill Development: Implement activities and exercises to improve strength, coordination, and motor control. Use age-appropriate play and functional activities to promote the acquisition of developmental milestones, such as crawling, walking, and climbing.
- Gait and Mobility Training: Address gait abnormalities and mobility limitations through specific interventions, such as treadmill training, balance exercises, and obstacle courses. Use assistive devices, such as walkers or orthotics, to support safe and efficient movement.
- Postural Control and Alignment: Work on improving postural control and alignment through exercises that target core strength, trunk stability, and symmetry. Use positioning aids and adaptive seating to promote best posture during daily activities.
- Range of Motion and Flexibility: Implement range of motion exercises and stretching routines to prevent contractures and maintain joint flexibility. Teach caregivers how to perform these exercises at home to ensure regular practice.
- Aquatic Therapy: Consider incorporating aquatic therapy into the treatment plan to provide a supportive and low-impact environment for motor skill practice. The buoyancy and resistance of water can facilitate movement and improve strength and endurance.
- Adaptive Equipment and Orthotics: Recommend and train the individual and caregivers in the use of adaptive equipment, such as standers, gait trainers, and mobility aids. Collaborate with orthotists to design and fit custom orthotic devices to support proper alignment and function.
- Collaboration with Other Professionals: Work closely with occupational therapists, speech-language pathologists, and educators to ensure a comprehensive and coordinated approach to intervention. Share information and strategies to support the individual's participation and progress across settings.
Caregiver Suggestions
- Education and Training: Attend educational workshops and training sessions to learn about Friedreich's Ataxia, its management, and the latest research findings. Seek out resources from reputable organizations, such as the Friedreich's Ataxia Research Alliance (FARA) and NORD, to stay informed and empowered.
- Care Coordination: Maintain organized records of the individual's medical history, medications, and therapy reports. Coordinate care among various healthcare providers and specialists to ensure a comprehensive and cohesive approach to management.
- Advocacy: Advocate for the individual's needs and rights in educational, medical, and community settings. Participate in Individualized Education Program (IEP) meetings and collaborate with school personnel to ensure appropriate accommodations and support services are in place.
- Home Modifications: Make necessary modifications to the home environment to enhance safety, accessibility, and independence. Install ramps, grab bars, and adaptive equipment as needed to facilitate mobility and self-care activities.
- Respite Care: Seek out respite care services to provide temporary relief from caregiving responsibilities. Engage trusted family members, friends, or professional caregivers to assist with care and allow for self-care and stress management.
- Self-Care and Stress Management: Prioritize self-care activities, such as exercise, relaxation techniques, and hobbies, to maintain physical and emotional well-being. Join support groups or seek counseling to connect with other caregivers and address the unique challenges of caring for an individual with FA.
- Financial Planning: Investigate financial assistance programs, such as Medicaid waivers, Supplemental Security Income (SSI), and grants from non-profit organizations, to help cover the costs associated with medical care, therapies, and adaptive equipment.
- Transition Planning: Plan for the individual's future needs, including transitioning to adult services, long-term care options, and legal considerations, such as guardianship and special needs trusts. Work with a social worker or case manager to navigate the complex system of adult services and ensure continuity of care.
Educational Strategies
- Individualized Education Programs (IEPs): Develop individualized education programs tailored to the specific needs of students with FA.
- Special Education Services: Provide specialized instruction and support services to address learning challenges and promote academic progress.
- Assistive Technology in Education: Integrate assistive technology into the classroom to support communication, learning, and independence.
- Visual Supports: Use visual aids, such as pictures, schedules, and social stories, to enhance understanding and communication.
Extended Information
Challenges and Considerations
Caregiver Burden
Caring for an individual with FA can be physically, emotionally, and financially demanding for caregivers. It is essential to provide support and resources to caregivers to prevent burnout and promote their well-being.
Medical Complexity
Managing the multiple health issues associated with FA can be complex and require a multidisciplinary approach involving various healthcare professionals.
Communication Barriers
Significant speech and language delays present a challenge for individuals with FA, highlighting the need for early intervention with AAC devices and alternative communication strategies.
Behavioral Challenges
Hyperactivity, anxiety, and challenging behaviors can impact learning, social interactions, and daily living activities.
Long-Term Care
Individuals with FA require lifelong support and supervision, and planning for long-term care needs is crucial.
Pathological Insights
The absence or abnormal version of frataxin disrupts mitochondrial function, leading to the degeneration of nerve tissue in the spinal cord and peripheral nerves, affecting coordination, muscle strength, and sensory processing.
Genetic and Environmental Factors
FA is primarily genetic, caused by a mutation in the FXN gene. Environmental factors may influence the severity of symptoms but are not considered the primary cause.
Clinical Presentation and Disease Progression
The clinical presentation of FA varies widely, and disease progression can be unpredictable. Some individuals may experience a plateau in development, while others may show gradual improvement over time.
Differential Diagnosis
Other conditions that may present with similar symptoms to FA include:
Support and Resources
-
Friedreich's Ataxia Research Alliance (FARA):
-
National Organization for Rare Disorders (NORD):
-
Genetics Home Reference - NIH:
-
MedlinePlus - NIH:
-
Orphanet:
References
- https://rarediseases.org/rare-diseases/friedreichs-ataxia/
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Friedreich's Ataxia?
What does Friedreich's Ataxia do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.