Introduction
Muscular Dystrophy (MD) encompasses a group of genetic disorders characterized by progressive muscle weakness and degeneration. Each type presents with distinct patterns of muscle involvement, age of onset, and rate of progression. Diagnosis relies on clinical evaluation, genetic testing, and sometimes muscle biopsy. Management requires a multidisciplinary approach focused on maintaining function, managing complications, and supporting quality of life through therapeutic interventions and assistive technologies.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Variable
- Rarity Classification: Medium
- Typical Onset: Birth
- Gender Impact: Mostly Men
- Progressive/Degenerative: Yes
- Seizure Prevalence: Variable (Subtype)
- Population Trend: Stable
Pathophysiology
~30 genetic origins of various onset; highly prevalent, low undestanding and prognosis especially among men.
AAC Considerations
Recommended Access Modalities: All - Progression
Patient Advocacy & Support Organizations

Muscular Dystrophy
Demographic Information
- Incidence: Varies by type; for example, Duchenne Muscular Dystrophy (DMD) occurs in approximately 1 in 3,500 male births.
- Prevalence: Approximately 1 in 5,000 individuals worldwide, varying by type.
- Gender: Duchenne and Becker types primarily affect males; other types can affect both genders.
- Onset Age: Varies by type; Duchenne typically presents in early childhood, while others like Myotonic Dystrophy may present in adolescence or adulthood.
Coding
- ICD-11: 8C71
- ICD-10-CM: G71.09
- OMIM: Varies by type; for example, Duchenne Muscular Dystrophy is OMIM 310200.
- UMLS: C0026850
- MeSH: D009136
- GARD: 63
Quick Reference
| Quick Facts | Details |
|---|---|
| Incidence | Varies by type; Duchenne MD ~1 in 3,500 male births; Becker MD ~1 in 18,000-30,000 male births |
| Prevalence | Approximately 1 in 5,000 individuals worldwide (all types combined) |
| Gender Distribution | Duchenne & Becker primarily affect males (X-linked); other types affect both genders |
| Primary Age of Onset | Varies: Duchenne (early childhood 2-6 years), Becker (later childhood/adolescence), Myotonic (adolescence/adulthood) |
| AT/AAC Requirements | Moderate to High - Progressive condition; increasing need for mobility aids, respiratory support, and AAC as disease advances |
Medical Features and Pathophysiology
Etiology
Muscular Dystrophy (MD) encompasses a group of genetic disorders characterized by progressive muscle weakness and degeneration. The etiology varies by type but generally involves mutations in genes responsible for muscle structure and function. For instance, Duchenne and Becker Muscular Dystrophy are caused by mutations in the dystrophin gene, which is essential for muscle fiber integrity.
Pathology
MD is marked by the progressive loss of muscle fibers, replaced by fat and connective tissue. The pathological changes vary by type and can affect different muscle groups. In Duchenne Muscular Dystrophy, the absence of dystrophin leads to repeated cycles of muscle damage and repair, ultimately resulting in muscle fiber loss and replacement by fibrotic and fatty tissue.
Symptoms
- Early Symptoms:
- Delayed motor milestones (e.g., walking, running)
- Muscle weakness, particularly in the pelvic and shoulder girdles
- Gower’s sign (difficulty rising to a standing position)
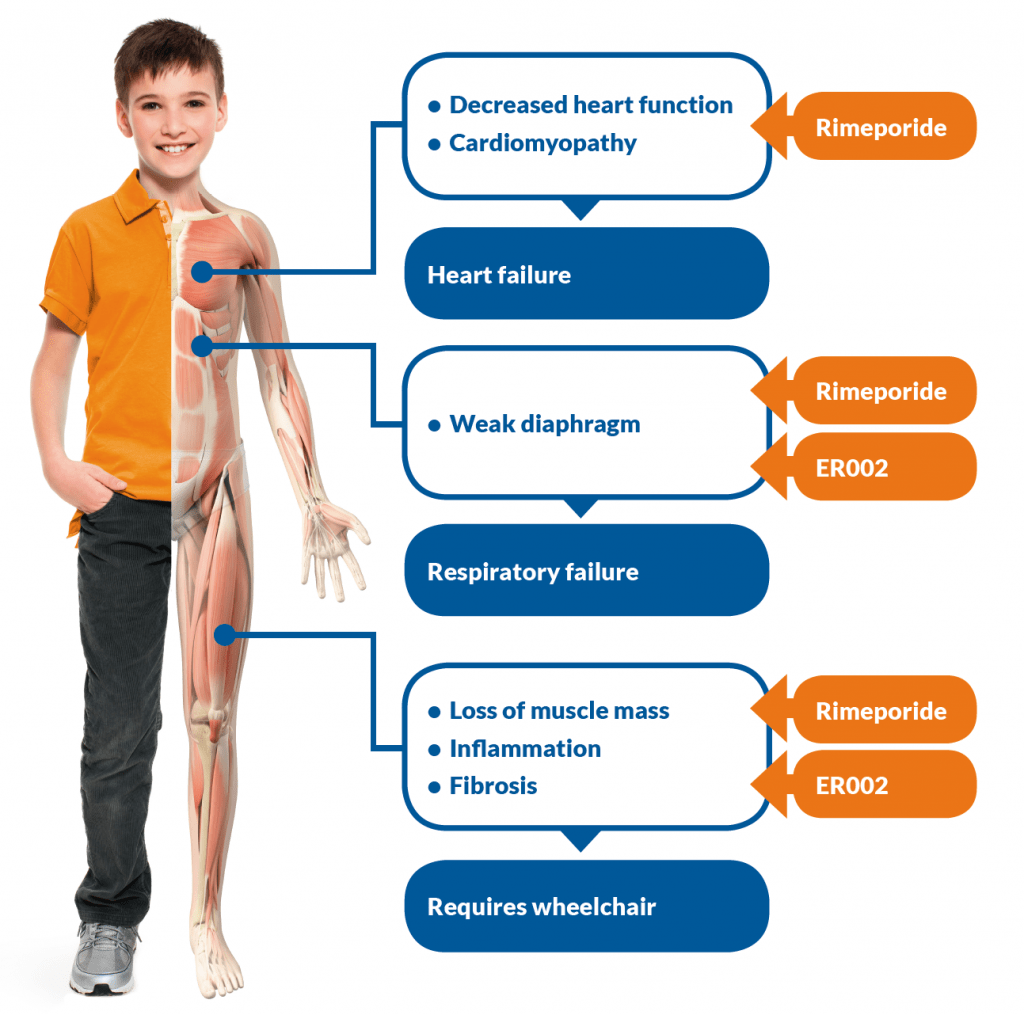
- Progressive Symptoms:
- Worsening muscle weakness and atrophy
- Respiratory difficulties due to involvement of respiratory muscles
- Cardiomyopathy and cardiac arrhythmias
- Contractures and scoliosis
- Cognitive impairment in some types, such as Duchenne
Diagnosis
Diagnosis of MD involves a combination of clinical evaluation, family history, genetic testing, and muscle biopsy. Genetic testing can identify specific mutations responsible for different types of MD. Muscle biopsy may show characteristic changes such as fiber size variation, necrosis, and fibrosis. Creatine kinase levels are often elevated in the blood, indicating muscle damage.
Assistive Suggestions and Requirements
Requirement Percentage for Assistive Technology
A high percentage of individuals with MD will require assistive technology due to progressive muscle weakness and loss of function.
Assistive Technology Suggestions
- Mobility Aids:
- Wheelchairs: Both manual and powered, depending on the severity of the condition.
- Scooters: For those who have some mobility but need assistance for longer distances.
- Communication Aids:
- Voice Amplifiers: To assist with weak speech.
- Speech Generating Devices (SGDs): For those who lose the ability to speak clearly.
- Home Modifications:
- Ramps and Stairlifts: To improve accessibility within the home.
- Grab Bars and Handrails: To enhance safety and independence.
- Adjustable Beds and Reclining Chairs: To improve comfort and ease of movement.
- Feeding Aids:
- Adaptive Utensils and Plates: Designed for individuals with reduced dexterity and strength.
Access Modalities
- Switch Access: For individuals with severe motor impairments to control communication devices and computers.
- Eye-Tracking Systems: Beneficial for those who retain eye movement control but have lost most other motor functions.
- Touchscreen Devices: Useful in the earlier stages when fine motor skills are still relatively preserved.
Care Management and Therapeutic Techniques
Aims
- To manage symptoms and maintain the highest possible level of independence and quality of life.
- To provide supportive care and address complications through a multidisciplinary approach.
- To offer education and support to patients and caregivers.
SLP Suggestions
- Assessment and Intervention:
- Regular Speech and Swallowing Assessments: To monitor changes and adjust therapy plans accordingly.
- Swallowing Techniques: Teaching techniques to ensure safe swallowing and reduce the risk of aspiration.
- Voice Therapy: Exercises to maintain voice strength and clarity.
- Augmentative and Alternative Communication (AAC):
- Introduction of AAC devices early in the disease progression to ensure familiarity and ease of use as the disease progresses.
Special Educator Suggestions
- Cognitive Rehabilitation:
- Activities designed to enhance executive function, memory, and attention.
- Use of memory aids, such as notebooks or electronic organizers.
- Behavioral Strategies:
- Structured routines to manage apathy and maintain engagement in activities.
- Positive reinforcement to encourage participation and effort in tasks.
Occupational Therapist Suggestions
- Daily Living Skills:
- Training in the use of adaptive equipment for self-care activities (e.g., dressing, grooming).
- Techniques to conserve energy and manage fatigue.
- Home and Environmental Modifications:
- Assessing and modifying the home environment to ensure safety and accessibility.
- Recommendations for ergonomic furniture and tools to support independence.
Recommendations on AAC and Other Details
- Text-Based AAC:
- Use of text-to-speech apps and devices for individuals who retain good literacy skills.
- Predictive text features to speed up communication.
- Symbol-Based AAC:
- For individuals with cognitive impairments affecting literacy, symbol-based systems like Picture Communication Symbols (PCS) can be useful.
- Dynamic display devices that can grow with the user’s needs.
Additional Information
Early diagnosis enables timely intervention and family planning. Regular monitoring by neurologists, cardiologists, pulmonologists, and rehabilitation specialists helps anticipate and manage complications. Physical therapy maintains mobility and prevents contractures, while respiratory support becomes increasingly important as the disease progresses. Patient and caregiver education through support groups and community resources provides practical guidance for daily challenges.
Extended Information
Pathological Insights and Disease Mechanism
Muscular Dystrophy (MD) encompasses a diverse group of genetic disorders characterized by progressive muscle weakness and degeneration. Each type of MD is caused by mutations in specific genes that affect muscle function. For example, Duchenne Muscular Dystrophy (DMD) and Becker Muscular Dystrophy (BMD) are caused by mutations in the dystrophin gene, which encodes the protein dystrophin. Dystrophin is crucial for maintaining the structural integrity of muscle fibers. In the absence of functional dystrophin, muscle fibers are prone to damage and degeneration, leading to the characteristic symptoms of DMD and BMD. Other types of MD, such as Myotonic Dystrophy and Facioscapulohumeral Muscular Dystrophy, are caused by different genetic mutations that disrupt various aspects of muscle cell function.
Genetic and Environmental Factors
While MD is primarily a genetic disorder, the severity and progression of symptoms can be influenced by various factors. Genetic modifiers, such as polymorphisms in other genes, can affect the disease course. Environmental factors, including physical activity and nutritional status, can also play a role in managing symptoms and maintaining muscle function. Genetic counseling is important for affected families to understand the inheritance patterns and risks of recurrence in future generations.
Clinical Presentation and Disease Progression
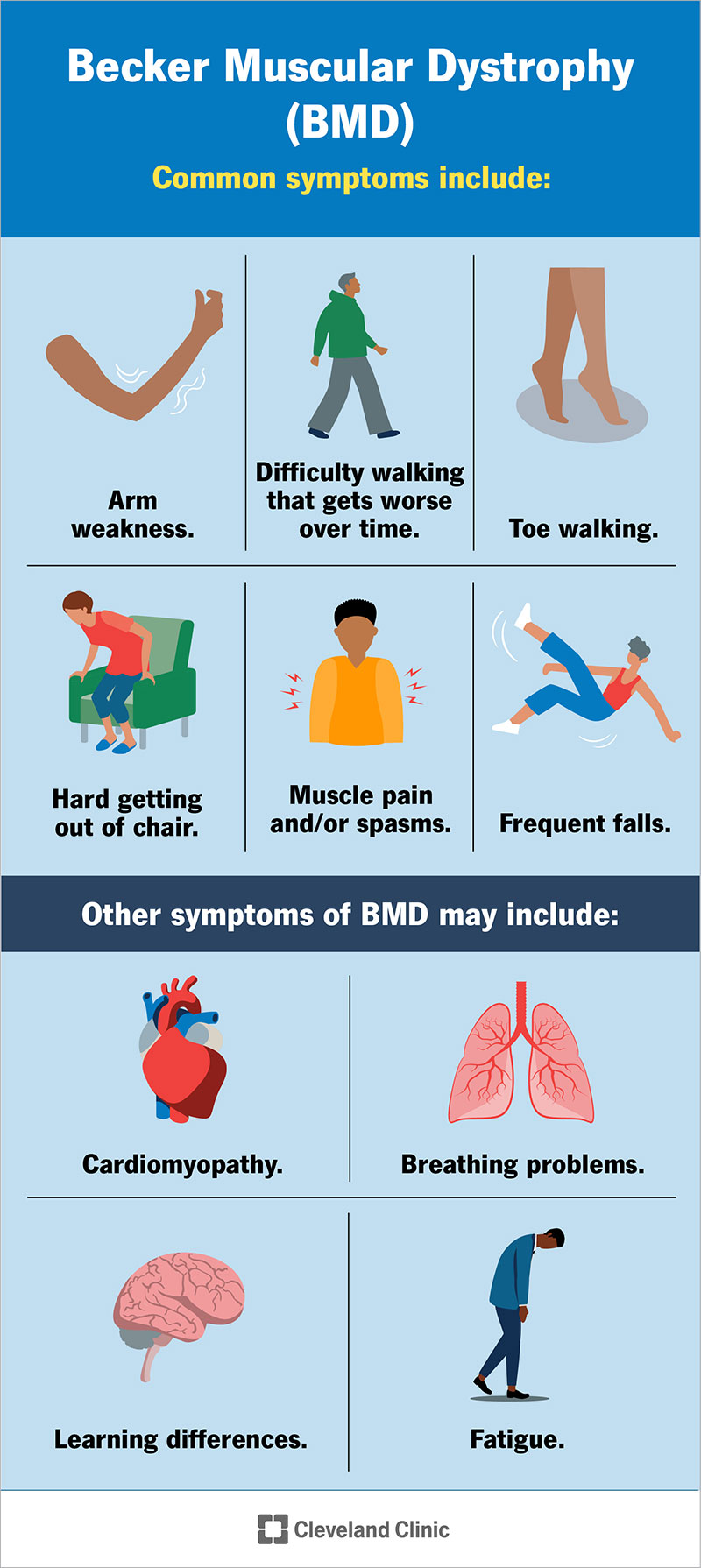
The clinical presentation of MD varies widely depending on the type and severity of the disorder. In Duchenne Muscular Dystrophy, symptoms typically appear in early childhood. Affected boys may experience delays in motor milestones such as walking and running. Muscle weakness initially affects the pelvic and shoulder girdles, leading to difficulties in climbing stairs, getting up from the floor, and running. Gower’s sign, a characteristic maneuver used to rise from the floor, is often observed. As the disease progresses, muscle weakness becomes more generalized, and affected individuals may lose the ability to walk by their early teens. Respiratory and cardiac complications become prominent in later stages. In contrast, Becker Muscular Dystrophy presents with milder symptoms and a slower progression, with affected individuals maintaining ambulation into adulthood.
Differential Diagnosis and Overlapping Syndromes
The diagnosis of MD involves differentiating it from other neuromuscular disorders that can present with similar symptoms. Conditions such as congenital myopathies, metabolic myopathies, and spinal muscular atrophies need to be considered. A thorough clinical evaluation, including detailed history, physical examination, and appropriate genetic testing, is essential for an accurate diagnosis. Muscle biopsy may be performed to assess the histopathological changes characteristic of MD and to rule out other
conditions.
Therapeutic Interventions and Symptom Management
Currently, there is no cure for MD, and treatment focuses on managing symptoms and improving quality of life. Corticosteroids, such as prednisone and deflazacort, are commonly used to slow the progression of muscle weakness in Duchenne Muscular Dystrophy. These medications can help maintain muscle strength and function, delay the onset of respiratory and cardiac complications, and improve overall survival. Physical therapy is essential for maintaining mobility, preventing contractures, and managing pain. Regular monitoring of respiratory and cardiac function is crucial, as interventions such as non-invasive ventilation and medications for heart failure may be needed. Nutritional support and management of swallowing difficulties are also important aspects of care.
Research and Future Directions
Research into MD is focused on understanding the underlying genetic and molecular mechanisms and developing targeted therapies. Gene therapy approaches, such as exon skipping and gene editing, aim to restore the production of functional dystrophin in patients with Duchenne Muscular Dystrophy. Clinical trials investigating these therapies have shown promising results, with some treatments already approved for use. Other areas of research include the development of anti-inflammatory and anti-fibrotic agents to mitigate muscle damage and the exploration of stem cell-based therapies to regenerate muscle tissue. Advances in genetic testing and molecular diagnostics are improving the accuracy of diagnosis and enabling personalized treatment approaches.
Support and Resources
Patients with MD and their caregivers can benefit from various support resources. Organizations such as the Muscular Dystrophy Association (www.mda.org) and the Duchenne Family Support Group (www.duchennefamilysupport.org) offer educational materials, support networks, and advocacy for those affected by the disease. These organizations also fund research initiatives aimed at finding a cure and improving the quality of life for individuals with MD. Support groups, both in-person and online, provide a platform for patients and caregivers to share experiences, receive emotional support, and access practical advice.
Gene therapy approaches, exon skipping, and improved corticosteroid regimens represent promising avenues for treatment. Clinical trials continue to evaluate novel therapies aimed at slowing disease progression and improving functional outcomes.
References
- Emery, A. E. H. (2002). The muscular dystrophies. The Lancet, 359(9307), 687-695.
- Bushby, K., Finkel, R., Birnkrant, D. J., Case, L. E., Clemens, P. R., Cripe, L., ... & DMD Care Considerations Working Group. (2010). Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. The Lancet Neurology, 9(1), 77-93.
- Mercuri, E., & Muntoni, F. (2013). Muscular dystrophies. The Lancet, 381(9869), 845-860.
- https://www.ohsu.edu/sites/default/files/2018-11/AAC%20for%20People%20with%20Progressive%20Neuromuscular%20Disease.pdf
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Muscular Dystrophy?
What does Muscular Dystrophy do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.