Introduction
Neonatal encephalopathy primarily results from hypoxic-ischemic injury during the perinatal period, though other etiologies include infection, stroke, and metabolic disorders. Reduced oxygen delivery and blood flow trigger a cascade of neuronal damage affecting brain structure and function. Clinical severity ranges from mild transient symptoms to profound neurological impairment. Diagnosis combines clinical assessment with laboratory testing and neuroimaging. Therapeutic hypothermia initiated within 6 hours of birth has significantly improved outcomes for moderate to severe hypoxic-ischemic encephalopathy. Approximately 40-60% of survivors experience long-term motor, cognitive, or communication impairments requiring assistive technology and ongoing therapeutic support.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Prenatal
- Pathology: Variable
- Rarity Classification: Medium
- Typical Onset: Birth
- Gender Impact: Either Gender
- Seizure Prevalence: Variable (Subtype)
- Population Trend: Decreasing
Pathophysiology
Root cause is generally hypoexia, but can be secondary to infection, stroke, trauma, birth asphyxia, and much more.
AAC Considerations
Recommended Access Modalities: All - Variable
Additional Clinical Notes
Neonatal asphyxiation that can take various forms; a bucket term really that can even include CP. Incidence much higher in the developing world
Neonatal Encephalopathy
Formal Name: Neonatal Hypoxic-Ischemic Encephalopathy (HIE)
Demographic Information
- Incidence: Approximately 1-6 per 1000 live births in developed countries
- Prevalence: Varies significantly based on region and quality of neonatal care
- Gender: No significant gender preference
- Onset Age: Birth or shortly after
Coding
- ICD-11: 8A03.0
- ICD-10-CM: P91.819
- OMIM: 603545
- UMLS: C0206081
- MeSH: D019966
- GARD: 0007607
Medical Features and Pathophysiology
Etiology
Neonatal encephalopathy is primarily caused by hypoxic-ischemic events during the perinatal period, which involve a reduction in oxygen (hypoxia) and blood flow (ischemia) to the infant's brain. These events can occur due to complications such as placental abruption, umbilical cord accidents, uterine rupture, or severe maternal hypotension. Other contributing factors can include intrauterine infections, metabolic disorders, trauma during delivery, and congenital abnormalities.
Pathology
The pathophysiology of neonatal encephalopathy involves a cascade of biochemical events triggered by hypoxia-ischemia, leading to neuronal injury and death. Key pathological findings include:
- Neuronal Necrosis: Death of neurons due to lack of oxygen and nutrients.
- Gliosis: Proliferation of glial cells in response to brain injury.
- Cystic Encephalomalacia: Formation of cystic cavities in the brain as a result of extensive tissue loss.
- White Matter Injury: Damage to the brain's white matter, often seen in the form of periventricular leukomalacia (PVL).
Symptoms
Symptoms of neonatal encephalopathy can vary widely in severity, depending on the extent and duration of the hypoxic-ischemic insult. They are typically classified into three stages:
Stage I (Mild):
- Hyperalertness or irritability
- Hypertonia (increased muscle tone)
- Poor feeding
- Increased Moro reflex
Stage II (Moderate):
- Lethargy
- Hypotonia (decreased muscle tone)
- Diminished reflexes
- Seizures
- Apnea (temporary cessation of breathing)
- Weak or absent Moro reflex
Stage III (Severe):
- Coma or stupor
- Flaccid paralysis
- Absent reflexes
- Prolonged seizures
- Respiratory failure
- Abnormal heart rate and blood pressure
Diagnosis
Diagnosing neonatal encephalopathy involves a combination of clinical assessment, laboratory tests, and imaging studies. Key diagnostic methods include:
Clinical Assessment:
- Apgar Score: Evaluates the newborn's heart rate, respiratory effort, muscle tone, reflexes, and skin color at 1 and 5 minutes after birth.
- Neurological Examination: Assesses level of consciousness, muscle tone, reflexes, and response to stimuli.
Laboratory Tests:
- Blood Gas Analysis: Measures levels of oxygen, carbon dioxide, and pH in the blood to assess the severity of hypoxia and acidosis.
- Electrolyte Levels: Monitors for abnormalities that can indicate metabolic disturbances.
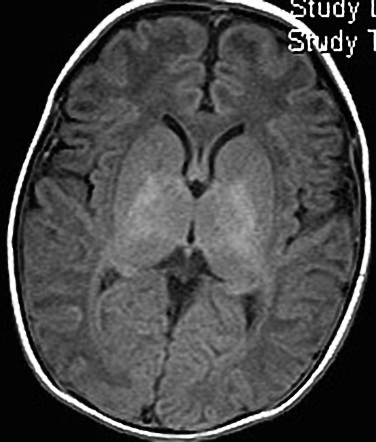
Imaging Studies:
- Magnetic Resonance Imaging (MRI): The gold standard for detecting brain injury, particularly useful for identifying white matter damage, hemorrhages, and cystic changes.
- Computed Tomography (CT) Scan: Useful for detecting acute hemorrhages and structural abnormalities.
- Cranial Ultrasound: Often used in the neonatal intensive care unit (NICU) for ongoing monitoring of brain structure and detecting intraventricular hemorrhage.
Electroencephalography (EEG):
- Used to detect abnormal brain activity, including seizures and suppressed background activity, which are common in neonatal encephalopathy.
Assistive Suggestions and Requirements
Requirement Percentage for Assistive Technology
Approximately 40-60% of survivors of neonatal encephalopathy may require assistive technology due to varying degrees of motor, cognitive, and communication impairments.
Assistive Technology Suggestions
Mobility Aids:
- Wheelchairs and Walkers: For children with significant motor impairments to facilitate mobility and independence.
- Standers and Gait Trainers: To support weight-bearing and promote walking practice in children with lower extremity weakness.
Communication Aids:
- Augmentative and Alternative Communication (AAC) Devices: For children with speech impairments, including dedicated communication devices, apps on tablets, and speech-generating devices.
- Eye-Gaze Systems: For children with severe motor impairments who can control communication devices using eye movements.
Feeding and Nutritional Aids:
- Specialized Feeding Equipment: Such as adapted utensils, cups, and plates for children with difficulties in hand function.
- Gastrostomy Tubes (G-tubes): For children with severe swallowing difficulties to ensure adequate nutrition and hydration.
Environmental Modifications:
- Grab Bars and Handrails: Installed in the home to assist with transfers and mobility.
- Adjustable Beds and Positioning Aids: To provide proper support and comfort, especially for children with significant physical disabilities.
Therapeutic Equipment:
- Therapeutic Exercise Equipment: Such as therapy balls, mats, and resistance bands for physical therapy at home.
- Sensory Integration Tools: Including weighted blankets, swings, and tactile toys to support children with sensory processing difficulties.
Access Modalities
Switch Access:
- For children with severe motor impairments, allowing control of devices through simple switches activated by any reliable body movement (e.g., head, chin, foot).
Voice-Controlled Systems:
- Beneficial for children who retain good vocal strength but have limited physical abilities, enabling control of smart home devices and communication aids through voice commands.
Touchscreen Devices:
- Useful for children with adequate hand dexterity, enabling access to educational apps, communication tools, and recreational activities.
Care Management and Therapeutic Techniques
Aims
The primary aims of care management for children with neonatal encephalopathy include optimizing neurological outcomes, preventing complications, and enhancing quality of life through a multidisciplinary approach.
SLP Suggestions
Assessment and Intervention:
- Regular Speech and Swallowing Assessments: To monitor changes in function and adapt therapy plans accordingly.
- Swallowing Techniques: Teaching safe swallowing techniques to reduce the risk of aspiration and improve oral intake.
- Voice Therapy: Exercises to strengthen the voice and improve clarity, tailored to the child's specific needs.
Augmentative and Alternative Communication (AAC):
- Introduction of AAC Early: Introducing AAC devices early in the disease progression to ensure familiarity and ease of use as the child grows.
- Customized AAC Systems: Tailoring AAC systems to the child's cognitive and physical abilities, ensuring they are user-friendly and effective.
Special Educator Suggestions
Individualized Education Plans (IEP):
- Developing IEPs: Creating comprehensive IEPs that address the child's specific learning needs, incorporating goals for cognitive, motor, and communication skills.
- Multisensory Teaching Methods: Using a combination of visual, auditory, and tactile inputs to enhance learning and engagement.
Cognitive Rehabilitation:
- Memory Aids: Implementing tools like notebooks, electronic organizers, and reminder systems to support memory and executive function.
- Behavioral Strategies: Establishing structured routines and using positive reinforcement to encourage participation and effort in educational tasks.
Occupational Therapist Suggestions
Daily Living Skills:
- Adaptive Equipment Training: Teaching the use of adaptive equipment for self-care activities, such as dressing and grooming.
- Energy Conservation Techniques: Educating on methods to conserve energy and manage fatigue during daily activities.
Home and Environmental Modifications:
- Safety Assessments: Conducting home assessments to identify and address potential safety hazards.
- Ergonomic Furniture Recommendations: Suggesting ergonomic furniture and tools to support independence and comfort in the home environment.
Recommendations on AAC and Other Details
Text-Based AAC:
- Text-to-Speech Apps and Devices: Utilizing text-to-speech technology for children who retain good literacy skills, with features like predictive text to enhance communication speed.
Symbol-Based AAC:
- Picture Communication Symbols (PCS): For children with cognitive impairments affecting literacy, using symbol-based systems that are intuitive and easy to understand.
- Dynamic Display Devices: Devices that can grow and adapt to the child's changing needs, providing a flexible communication solution.
Extended Information
Pathological Insights and Disease Mechanism
Neonatal encephalopathy is caused by a combination of factors that lead to hypoxia and ischemia during the perinatal period. These events trigger a series of biochemical reactions in the brain, resulting in energy failure, oxidative stress, inflammation, and excitotoxicity. The lack of oxygen and glucose disrupts cellular metabolism, leading to the accumulation of harmful substances like free radicals and lactic acid. This biochemical cascade ultimately causes neuronal injury and cell death, particularly in vulnerable areas such as the basal ganglia, thalamus, and cortical gray matter.
Genetic and Environmental Factors
While hypoxic-ischemic events are the primary cause, genetic factors may influence the susceptibility and severity of neonatal encephalopathy. Polymorphisms in genes involved in oxidative stress response, inflammation, and neuroprotection can affect the brain's ability to withstand and recover from hypoxic-ischemic injury. Environmental factors, such as maternal health and the quality of neonatal care, also play significant roles in outcomes.
Research and Future Directions
Current research explores neuroprotective agents beyond therapeutic hypothermia, refinement of cooling protocols, and regenerative medicine approaches including stem cell therapies. Biomarker development aims to improve early identification of at-risk infants and predict long-term outcomes.
Support and Resources
Organizations such as the Hypoxic Ischemic Encephalopathy Foundation (www.hiefoundation.org) and the United Cerebral Palsy Association (www.ucp.org) provide educational resources, family support networks, and research advocacy. Online and in-person support groups connect families navigating similar challenges.
References
This section provides key research and clinical resources.
Clinical Studies & Treatment
- , et al. (2019). Neonatal Encephalopathy: Need for Recognition of Multiple Etiologies for Optimal Management. Frontiers in Pediatrics. https://doi.org/10.3389/fped.2019.00142 Link [PDF]
Additional Resources
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Neonatal Encephalopathy?
What does Neonatal Encephalopathy do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.