Introduction
Pitt-Hopkins Syndrome (PTHS) results from mutations in the TCF4 gene on chromosome 18q21.2, disrupting normal brain development. Affected individuals present with severe to profound intellectual disability, absent or minimal speech, distinctive facial features, episodic hyperventilation, and hypotonia. Diagnosis relies on genetic testing confirming TCF4 mutations. Approximately 80-90% require augmentative communication systems, with specific considerations needed for visual impairments that may limit eye-gaze access despite appropriate candidacy for this modality.
Comprehensive Overview of Pitt-Hopkins Syndrome
Demographic Information
- Incidence: Estimated at 1 in 34,000 to 1 in 41,000 births.
- Prevalence: Considered a rare disorder with cases reported worldwide.
- Gender: Affects both males and females equally, without a notable gender preference.
- Onset Age: Symptoms are typically identified in early childhood, around 2 to 4 years old, though some features may be noticeable earlier.
Coding
- ICD-11: 5A00.3
- ICD-10-CM: Q87.89
- OMIM: 610954
- UMLS: C1834020
- MeSH: Not specifically listed.
- GARD: 9504
Medical Features and Pathophysiology
Etiology
Pitt-Hopkins Syndrome is caused by mutations in the TCF4 gene, located on chromosome 18q21.2. The TCF4 gene is responsible for encoding the transcription factor 4 protein, which is crucial for the development and function of the nervous system. Mutations in this gene lead to the disruption of various developmental processes, particularly those affecting the brain and nervous system.
Pathology
The pathophysiological mechanisms of Pitt-Hopkins Syndrome involve impaired neurogenesis, synaptogenesis, and overall neural connectivity due to the dysfunctional TCF4 protein. This results in a spectrum of cognitive, developmental, and physical abnormalities. The exact pathways and interactions remain an active area of research, aiming to understand how these genetic mutations translate into the clinical symptoms observed in PTHS patients.
Symptoms
- Intellectual Disability: Individuals with PTHS exhibit severe to profound intellectual disability. Cognitive development is significantly delayed, with many children never developing functional speech.
- Developmental Delays: Delays are evident in all developmental domains including gross and fine motor skills, speech and language, and social interaction.
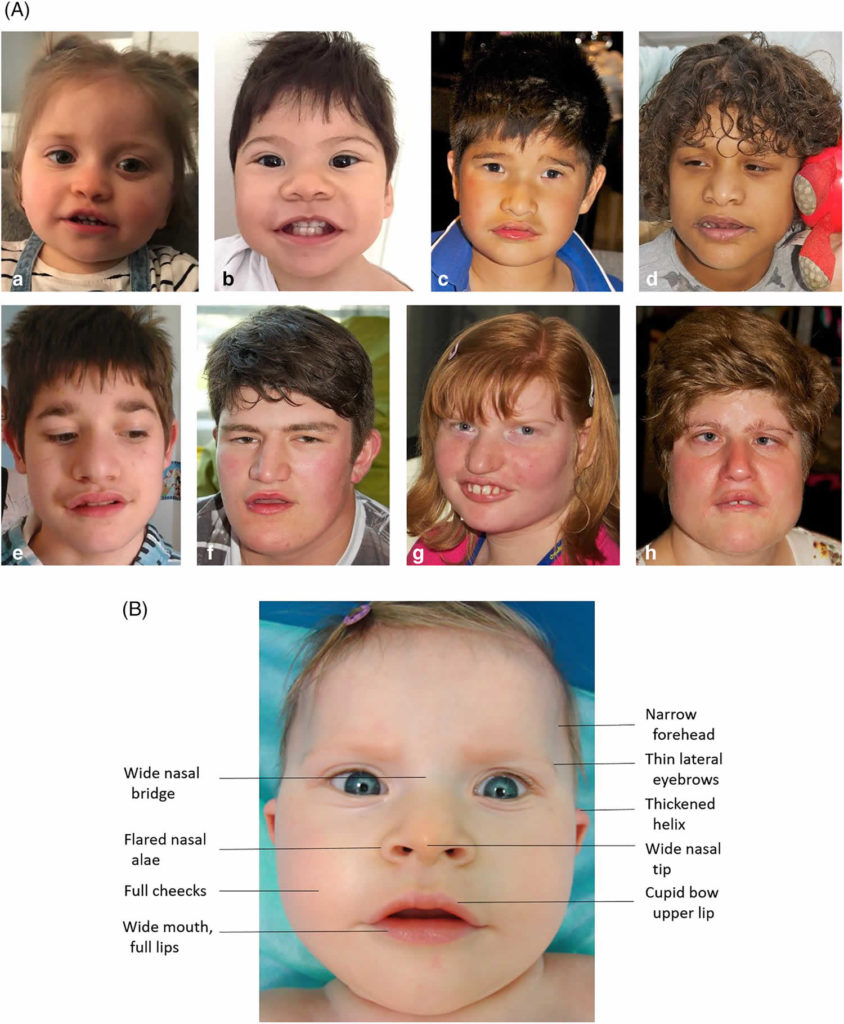
- Characteristic Facial Features: Distinct facial characteristics include deep-set eyes, a prominent forehead, a wide nasal bridge, a wide mouth with thick lips, and widely spaced teeth. These features become more pronounced with age.
- Breathing Abnormalities: Episodes of hyperventilation followed by apnea are common, often triggered by excitement or stress. These breathing irregularities can start in infancy or early childhood.
- Motor Dysfunction: Hypotonia (low muscle tone) and ataxia (lack of muscle coordination) are frequently observed, impacting both fine and gross motor skills.
- Behavioral Issues: Autism-like behaviors, hyperactivity, anxiety, and stereotypic movements (repetitive, non-functional movements) are common in children with PTHS.
- Gastrointestinal Issues: Constipation is a frequent problem due to hypotonia affecting the muscles of the digestive tract.
- Sleep Disturbances: Many children with PTHS have irregular sleep patterns, including difficulty falling asleep and frequent awakenings during the night.
- Seizures: Epilepsy is present in approximately 40-50% of individuals with PTHS, often beginning in childhood and requiring management with antiepileptic medications.
Diagnosis
- Genetic Testing: Confirmation of TCF4 gene mutations through whole exome sequencing or targeted genetic testing.
- Clinical Evaluation: Comprehensive assessment of symptoms, including developmental history, physical examination, and detailed medical history.
- Electroencephalogram (EEG): To detect abnormal brain wave patterns associated with seizures.
- Magnetic Resonance Imaging (MRI): To assess brain structure and identify any abnormalities in brain development.
Assistive Suggestions and Requirements
Requirement Percentage for Assistive Technology: Approximately 80-90% of individuals with PTHS will need assistive technology.
Assistive Technology Suggestions
- Augmentative and Alternative Communication (AAC) Devices:
- Eye-Tracking Technology: For non-verbal communication, enabling children to use their eyes to select words or symbols on a screen.
- Speech-Generating Devices (SGDs): Devices that produce spoken language based on input from the user, which can include touch screens, switches, or eye-tracking.
- Mobility Aids:
- Walkers and Gait Trainers: To support mobility and enhance independence in children with motor dysfunction.
- Wheelchairs: For children with significant mobility impairments, providing both manual and power options.
- Educational Tools:
- Adaptive Learning Software: Programs tailored to the individual’s cognitive level, incorporating visual and auditory stimuli to support learning.
- Sensory Integration Tools: Items such as weighted blankets, fidget toys, and sensory mats to help manage sensory processing issues and improve focus.
Access Modalities
- Eye-Tracking Technology: Essential for individuals with severe motor impairments, enabling them to communicate and interact with their environment using only their eye movements.
- Switch Access: For those with limited hand dexterity, switches can be used to operate communication devices, computers, and other technology.
- Touchscreen Devices: Beneficial for individuals with adequate hand control, allowing them to interact directly with communication and educational tools.
Care Management and Therapeutic Techniques
- Enhance Communication: Improve the ability to express needs and interact with others through the use of AAC devices and speech therapy.
- Support Motor Function: Enhance mobility and coordination through physical therapy and the use of assistive devices.
- Manage Medical Issues: Address and manage gastrointestinal issues, sleep disturbances, and seizures with appropriate medical interventions.
- Behavioral Support: Implement strategies to manage anxiety, hyperactivity, and autism-like behaviors, improving overall quality of life.
SLP Suggestions
- Assessment and Intervention:
- Regular Speech and Swallowing Assessments: To monitor changes and adjust therapy plans accordingly.
- Swallowing Techniques: Teaching techniques to ensure safe swallowing and reduce the risk of aspiration.
- Voice Therapy: Exercises to maintain voice strength and clarity.
- Augmentative and Alternative Communication (AAC):
- Introduction of AAC Devices: Early introduction to ensure familiarity and ease of use as the disease progresses.
- Customizing AAC Tools: Tailoring devices to the individual's specific needs, ensuring they are user-friendly and effective.
Special Educator Suggestions
- Cognitive Rehabilitation:
- Activities to Enhance Executive Function: Exercises designed to improve memory, attention, and problem-solving skills.
- Use of Memory Aids: Tools such as notebooks or electronic organizers to help manage daily tasks and improve independence.
- Behavioral Strategies:
- Structured Routines: Implementing consistent daily routines to manage behaviors and provide a sense of security.
- Positive Reinforcement: Encouraging participation and effort in educational and therapeutic activities through rewards and praise.
Occupational Therapist Suggestions
- Daily Living Skills:
- Adaptive Equipment Training: Teaching the use of tools and devices to assist with self-care activities such as dressing, grooming, and feeding.
- Energy Conservation Techniques: Strategies to manage fatigue and optimize participation in daily activities.
- Home and Environmental Modifications:
- Assessing and Modifying Home Environments: Ensuring safety and accessibility, including the installation of grab bars, handrails, and other modifications.
- Ergonomic Recommendations: Providing advice on furniture and tools that support independence and reduce physical strain.
Recommendations on AAC
- Text-Based AAC:
- Text-to-Speech Apps and Devices: Useful for individuals who retain good literacy skills, enabling them to communicate effectively.
- Predictive Text Features: Enhancing communication speed and efficiency.
- Symbol-Based AAC:
- Picture Communication Symbols (PCS): For individuals with cognitive impairments affecting literacy, symbol-based systems can be highly effective.
- Dynamic Display Devices: AAC devices that can adapt and grow with the user’s needs, providing a flexible communication solution.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Heritable
- Rarity Classification: Rare
- Typical Onset: Birth
- Gender Impact: Either Gender
- Seizure Prevalence: Yes (>90%)
- Population Trend: Stable
Pathophysiology
Autosomal dominant mutation of the TCF4 gene, which controls creation of a protein that is critically important for DNA transcription, causing an impact cascade. One typical example in Pitt Hopkins is the TCF4 protein deficiency leading to low expression of the ASCL1 protein because of impact to other genes, which is implicated in Pitt's hallmark respiratory complications.
AAC Considerations
Recommended Access Modalities: All - Variable
Additional Clinical Notes
Visual comorbidities reduce eye gaze access case here, despite frequent candidacy
Patient Advocacy & Support Organizations
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3366706/
Visual Aids and Graphics
- Genetic Pathway of TCF4 Gene Mutation: Diagram showing how mutations in the TCF4 gene disrupt normal brain development.
- Symptom Overview Chart: A chart categorizing the various symptoms of Pitt-Hopkins Syndrome, divided into cognitive, physical, and behavioral domains.
- Assistive Technology Options: Visual guide to different types of AAC devices, mobility aids, and educational tools recommended for PTHS.
Additional Notes
Research into PTHS explores the role of TCF4 in neural development and potential therapeutic targets. The TCF4 protein regulates expression of numerous genes critical for brain formation and function. Understanding downstream pathways affected by TCF4 deficiency may identify intervention points. Clinical trials and natural history studies help define the phenotypic spectrum and inform evidence-based management strategies.
Families and clinicians should monitor for respiratory episodes, which can be triggered by excitement or stress. Gastrointestinal issues, particularly constipation related to hypotonia, require proactive management. Seizure disorders affect approximately 40-50% of individuals, often requiring antiepileptic medications. Sleep disturbances are common and may benefit from behavioral interventions and environmental modifications.
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Pitt-Hopkins Syndrome?
What does Pitt-Hopkins Syndrome do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.