Introduction
Sturge-Weber Syndrome (SWS) is a congenital disorder caused by a mutation in the GNAQ gene, leading to vascular malformations in the skin, brain, and eyes. Symptoms include a facial port-wine stain, seizures, developmental delays, and glaucoma. Diagnosis involves clinical evaluation, neuroimaging, ophthalmologic examination, and genetic testing. Management requires a multidisciplinary approach, including medical treatments like antiepileptic drugs and glaucoma management, surgical interventions, and supportive therapies like physical, occupational, and speech therapy. Assistive technologies and home modifications can aid mobility and communication. Research into gene therapy and neurocognitive rehabilitation offers potential future treatments.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Mutation - Somatic
- Rarity Classification: Orphan
- Typical Onset: Birth
- Gender Impact: Either Gender
- Seizure Prevalence: Majority (50-90%)
- Population Trend: Unknown
Pathophysiology
GNAQ, wich encodes Guanine nucleotide-binding protein G(q) subunit alpha
AAC Considerations
Recommended Access Modalities: Touch,Switch
Additional Clinical Notes
Mild to severe intellectual ability plus glaucoma; age of onset of seizures is a key factor. Hallmark characteristic is a "port wine" birthmark on the face.
Patient Advocacy & Support Organizations
Sturge-Weber Syndrome (SWS)
Formal Name: Encephalotrigeminal Angiomatosis
Demographic Information:
- Incidence: Approximately 1 in 20,000 to 50,000 live births
- Prevalence: Roughly 1 in 20,000 to 50,000 people
- Gender: Affects both genders equally
- Onset Age: Present at birth, but symptoms can develop or worsen over time
Coding:
- ICD-11: LD20.0
- ICD-10-CM: Q85.8
- OMIM: 185300
- UMLS: C0038501
- MeSH: D013288
- GARD: 7640
Medical Features and Pathophysiology:
- Etiology: Sturge-Weber Syndrome (SWS) is a congenital disorder caused by a somatic mutation in the GNAQ gene. This mutation occurs randomly and is not inherited. The GNAQ gene mutation leads to abnormal blood vessel development and the characteristic vascular malformations seen in SWS.
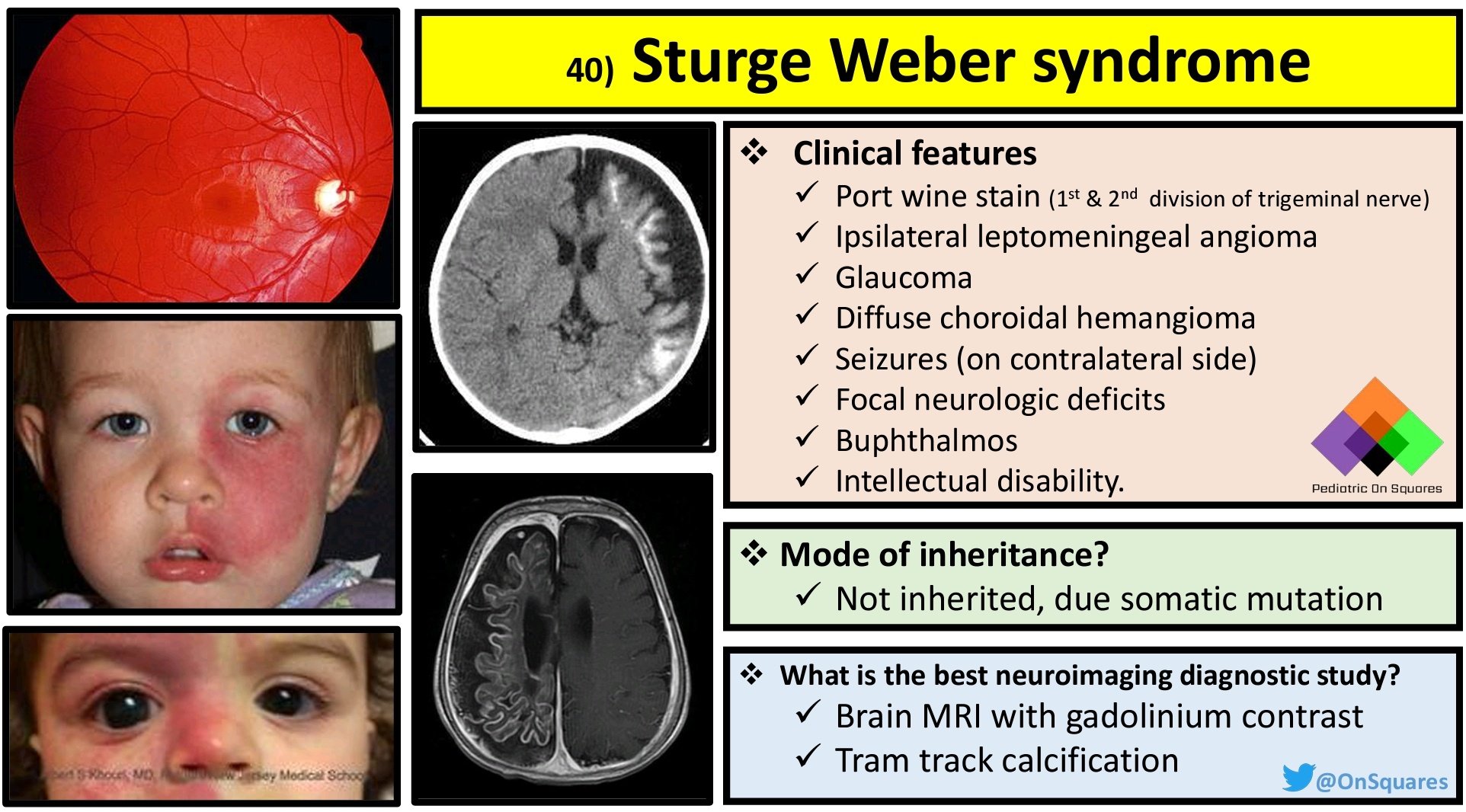
- Pathology: SWS is characterized by vascular malformations involving the skin, brain, and eyes. The hallmark feature is a facial port-wine stain (nevus flammeus), usually affecting one side of the face along the distribution of the trigeminal nerve. The brain may develop leptomeningeal angiomas, which can cause seizures, neurological deficits, and cognitive impairments. Ocular involvement can lead to glaucoma and other visual disturbances.
- Symptoms:
- Facial Symptoms:
- Port-wine stain (nevus flammeus) on the face
- Facial asymmetry
- Neurological Symptoms:
- Seizures (often starting in infancy)
- Hemiparesis (weakness on one side of the body)
- Developmental delays
- Intellectual disability
- Headaches
- Ocular Symptoms:
- Glaucoma
- Buphthalmos (enlargement of the eyeball)
- Visual field defects
- Facial Symptoms:
- Diagnosis: Diagnosis of SWS involves a combination of clinical evaluation and imaging studies:
- Clinical Examination: Assessment of facial port-wine stain, neurological deficits, and ocular abnormalities.
- Neuroimaging: MRI or CT scans to detect leptomeningeal angiomas and assess brain structure.
- Ophthalmologic Examination: Evaluation for glaucoma and other eye abnormalities.
- Genetic Testing: Identification of the GNAQ mutation can confirm the diagnosis.
Assistive Suggestions and Requirements
Requirement Percentage for Assistive Technology:
Many patients with SWS will benefit from assistive technology, particularly those with neurological and visual impairments.
Assistive Technology Suggestions:
- Mobility Aids:
- Canes or Walkers: To assist with balance and mobility for those with hemiparesis.
- Wheelchairs: For severe cases of mobility impairment.
- Communication Aids:
- Speech Generating Devices (SGDs): For individuals with speech difficulties.
- Voice Amplifiers: To assist with weak speech.
- Home Modifications:
- Grab Bars and Handrails: To enhance safety and prevent falls.
- Adjustable Beds: To improve comfort and ease of movement.
- Visual Aids:
- Magnifiers and Large Print Materials: For individuals with visual impairments.
- Screen Readers: For those with significant vision loss.
Access Modalities:
- Switch Access: For individuals with severe motor impairments to control communication devices and computers.
- Voice-Controlled Systems: Beneficial for those who retain good vocal strength.
- Touchscreen Devices: Useful for those with adequate hand dexterity.
Care Management and Therapeutic Techniques
Aims:
- To manage symptoms and maintain the highest possible level of independence and quality of life.
- To provide supportive care and address complications through a multidisciplinary approach.
- To offer education and support to patients and caregivers.
SLP Suggestions:
- Assessment and Intervention:
- Regular Speech and Swallowing Assessments: To monitor changes and adjust therapy plans accordingly.
- Swallowing Techniques: Teaching techniques to ensure safe swallowing and reduce the risk of aspiration.
- Voice Therapy: Exercises to maintain voice strength and clarity.
- Augmentative and Alternative Communication (AAC):
- Introduction of AAC devices early in the disease progression to ensure familiarity and ease of use as the disease progresses.
Special Educator Suggestions:
- Cognitive Rehabilitation:
- Activities designed to enhance executive function, memory, and attention.
- Use of memory aids, such as notebooks or electronic organizers.
- Behavioral Strategies:
- Structured routines to manage apathy and maintain engagement in activities.
- Positive reinforcement to encourage participation and effort in tasks.
Occupational Therapist Suggestions:
- Daily Living Skills:
- Training in the use of adaptive equipment for self-care activities (e.g., dressing, grooming).
- Techniques to conserve energy and manage fatigue.
- Home and Environmental Modifications:
- Assessing and modifying the home environment to ensure safety and accessibility.
- Recommendations for ergonomic furniture and tools to support independence.
Recommendations on AAC and other details:
Cognitive outcomes in Sturge-Weber syndrome vary considerably based on seizure control and neurological involvement. AAC selection should match the individual's cognitive profile.
- Text-Based AAC:
- Text-to-speech apps and devices for individuals who retain good literacy skills.
- Predictive text features to speed up communication.
- Symbol-Based AAC:
- Symbol-based systems like Picture Communication Symbols (PCS) for cognitive impairments affecting literacy.
- Dynamic display devices that adapt with the user's needs.
Additional Information
Sturge-Weber Syndrome is a complex congenital disorder that requires lifelong management and a multidisciplinary approach. Regular follow-ups with neurologists, ophthalmologists, dermatologists, and other healthcare professionals are essential. Patient and caregiver education, as well as access to community resources and support groups, can provide valuable assistance in managing this condition.
Extended Information
Pathological Insights and Disease Mechanism
Sturge-Weber Syndrome (SWS) is characterized by the presence of vascular malformations involving the skin, brain, and eyes. The somatic mutation in the GNAQ gene leads to abnormal blood vessel development, resulting in the characteristic port-wine stain on the face, leptomeningeal angiomas in the brain, and ocular abnormalities such as glaucoma. The exact mechanisms by which the GNAQ mutation leads to these vascular anomalies are still under investigation, but it is known to affect the signaling pathways that regulate blood vessel formation and function.
Genetic and Environmental Factors
SWS is caused by a somatic mutation in the GNAQ gene, which means the mutation occurs randomly during embryonic development and is not inherited from the parents. This mutation leads to mosaicism, where only a subset of the body's cells carries the mutation. The exact cause of the mutation is unknown, and there are no known environmental factors that increase the risk of developing SWS.
Clinical Presentation and Disease Progression
The clinical presentation of SWS varies widely among individuals. The hallmark feature is a facial port-wine stain, which is present at birth and can vary in size and intensity. Neurological symptoms, such as seizures and hemiparesis, typically develop in infancy or early childhood. Seizures can be difficult to control and may lead to progressive neurological decline. Ocular involvement, particularly glaucoma, can lead to vision loss if not managed appropriately. The course of the disease is variable, with some individuals experiencing stable symptoms and others having progressive neurological and ocular complications.
Differential Diagnosis and Overlapping Syndromes
Diagnosing SWS involves differentiating it from other conditions that can present with similar features. Conditions such as Klippel-Trenaunay syndrome, which also involves vascular malformations, and other neurocutaneous syndromes need to be considered. A thorough clinical evaluation, including detailed history, physical examination, and appropriate imaging studies, is essential for an accurate diagnosis. Genetic testing for the GNAQ mutation can confirm the diagnosis and differentiate SWS from other conditions.
Therapeutic Interventions and Symptom Management
The management of Sturge-Weber Syndrome (SWS) involves a multidisciplinary approach aimed at controlling symptoms, preventing complications, and improving the quality of life for affected individuals. The treatment plan is tailored to each patient's specific needs and may include medical, surgical, and supportive therapies.
Medical Management:
Antiepileptic Medications:
Seizures are a common and challenging symptom of SWS. Antiepileptic drugs (AEDs) are the first line of treatment to control seizures. The choice of medication depends on the type and frequency of seizures, as well as the patient's overall health and response to treatment. Common AEDs include carbamazepine, valproic acid, and levetiracetam. In some cases, a combination of medications may be necessary to achieve best seizure control.
Glaucoma Management:
Ocular involvement in SWS can lead to glaucoma, characterized by increased intraocular pressure (IOP) that can damage the optic nerve. Management of glaucoma includes medications such as beta-blockers, prostaglandin analogs, and carbonic anhydrase inhibitors to lower IOP. In cases where medications are insufficient, laser therapy or surgical interventions, such as trabeculectomy or glaucoma drainage implants, may be required.
Surgical Interventions:
Laser Therapy for Port-Wine Stains:
Pulsed dye laser therapy is the standard treatment for port-wine stains. It works by targeting the abnormal blood vessels in the skin, causing them to shrink and lighten the stain. Multiple treatment sessions are usually needed, and early intervention can improve outcomes.
Epilepsy Surgery:
For patients with intractable seizures that do not respond to medication, surgical options such as focal resection, hemispherectomy, or corpus callosotomy may be considered. These procedures aim to remove or disconnect the brain regions responsible for seizure activity, thereby reducing seizure frequency and severity.
Glaucoma Surgery:
Surgical interventions for glaucoma include trabeculectomy, which creates a new drainage pathway for aqueous humor, and glaucoma drainage implants, which help to control IOP. These procedures are considered when medical management fails to adequately control IOP.
Supportive Therapies:
Physical Therapy:
Physical therapy is essential for managing hemiparesis and other motor deficits. Therapists work with patients to improve strength, coordination, and mobility through targeted exercises and activities. Assistive devices such as braces, canes, or walkers may be recommended to enhance mobility and independence.
Occupational Therapy:
Occupational therapy focuses on helping patients perform daily activities and improve their functional abilities. Therapists may recommend adaptive equipment and techniques to assist with dressing, grooming, feeding, and other self-care tasks. Home modifications, such as grab bars and ramps, can also enhance safety and accessibility.
Speech and Language Therapy:
Speech and language therapy is important for patients with communication difficulties. Therapists work on improving speech clarity, language skills, and swallowing function. Augmentative and Alternative Communication (AAC) devices may be introduced to support communication for individuals with severe speech impairments.
Psychological Support:
Living with a chronic condition like SWS can be challenging for both patients and their families. Psychological support, including counseling and therapy, can help address emotional and behavioral issues, improve coping strategies, and enhance overall well-being.
Pain Management:
Pharmacological Approaches:
Pain management may include the use of analgesics, anti-inflammatory medications, or neuropathic pain agents, depending on the source and severity of pain. For example, botulinum toxin injections have been shown to be effective in managing spasticity and associated pain.
Non-Pharmacological Approaches:
Techniques such as physical therapy, relaxation exercises, and cognitive-behavioral therapy can also be beneficial in managing pain and improving quality of life.
Emerging Therapies:
Neurocognitive Rehabilitation:
New neurocognitive rehabilitation options are being developed and validated to address cognitive impairments associated with SWS. These interventions aim to improve cognitive function, enhance learning and memory, and support overall cognitive development.
Gene Therapy:
Research into gene therapy holds promise for future treatments of SWS. By targeting the underlying genetic mutation, gene therapy has the potential to correct the abnormal blood vessel development and prevent the associated complications.
Lifestyle and Home Management:
Regular Physical Activity:
Maintaining a high level of fitness through regular physical activity is important for overall health and well-being. Exercise can help improve cardiovascular health, muscle strength, and mental health.
Healthy Diet:
A balanced diet rich in nutrients supports overall health and can help manage some of the symptoms associated with SWS. It is important to consult with a healthcare provider or nutritionist to develop an appropriate diet plan.
Patient and Caregiver Education:
Education and Training:
Providing education and training to patients and caregivers is crucial for effective management of SWS. This includes information on the condition, treatment options, symptom management, and the use of assistive devices.
Support Groups:
Joining support groups can provide valuable emotional support and practical advice from others who are experiencing similar challenges. These groups can also offer a sense of community and reduce feelings of isolation.
Research and Future Directions:
Research into Sturge-Weber Syndrome is ongoing, with a focus on understanding the underlying mechanisms of the disease and developing new treatments. Advances in genetic research, neuroimaging, and therapeutic interventions hold promise for improving the management and outcomes of SWS. Clinical trials and research studies are essential for advancing knowledge and finding more effective treatments.
In conclusion, Sturge-Weber Syndrome is a complex condition that requires a comprehensive, multidisciplinary approach to management. Early diagnosis, individualized treatment plans, and ongoing support are essential for improving the quality of life for individuals with SWS. By staying informed about the latest research and treatment options, patients and caregivers can work with healthcare providers to achieve the best possible outcomes.
References
- Comi, A. M. (2011). Sturge-Weber syndrome. Handbook of Clinical Neurology, 100, 297-310.
- Shirley, M. D., Tang, H., Gallione, C. J., et al. (2013). Sturge-Weber syndrome and port-wine stains caused by somatic mutation in GNAQ. New England Journal of Medicine, 368(21), 1971-1979.
- Bodensteiner, J. B., & Roach, E. S. (1999). Sturge-Weber syndrome: Introduction and overview. Sturge-Weber Syndrome, 1-17.
- Lo, W., et al. (2016). Leveraging a Sturge-Weber Gene Discovery: An Agenda for Future Research. Pediatric Neurology. https://doi.org/10.1016/j.pediatrneurol.2015.11.009
- National Institute of Neurological Disorders and Stroke. Sturge-Weber Syndrome Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Sturge-Weber-Syndrome-Information-Page
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Sturge-Weber Syndrome?
What does Sturge-Weber Syndrome do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.