Introduction
Trisomy X is a genetic condition affecting females, caused by an extra X chromosome. Symptoms can range from mild to significant, including physical features like tall stature and reduced muscle tone, developmental delays, learning disabilities, and emotional or behavioral challenges. Diagnosis can be made prenatally or postnatally through karyotyping. Management requires a multidisciplinary approach, including speech-language pathologists, special educators, and occupational therapists. Assistive technology, such as communication aids, adaptive learning software, and physical therapy equipment, can be beneficial.

Trisomy X (47,XXX)
Demographic Information
- Incidence: Approximately 1 in 1,000 female births
- Prevalence: Estimated that around 10% of cases are clinically ascertained
- Gender: Affects only females
- Onset Age: Can be diagnosed prenatally or postnatally
Coding
- ICD-11: Q97.8
- ICD-10-CM: Q97.0
- OMIM: 300276
- UMLS: C0036866
- MeSH: D014310
- GARD: 7927
Medical Features and Pathophysiology
Etiology
Trisomy X is a genetic condition caused by the presence of an extra X chromosome in females (47,XXX instead of the typical 46,XX). This anomaly arises due to a random event during the formation of reproductive cells, known as nondisjunction. Advanced maternal age is a known risk factor for this condition.
Pathology
The extra X chromosome in trisomy X leads to a variable phenotype due to the overexpression of genes that escape X-inactivation. The exact genotype-phenotype relationships are not yet fully understood. The physical and psychological manifestations can range from mild to significant.
Symptoms
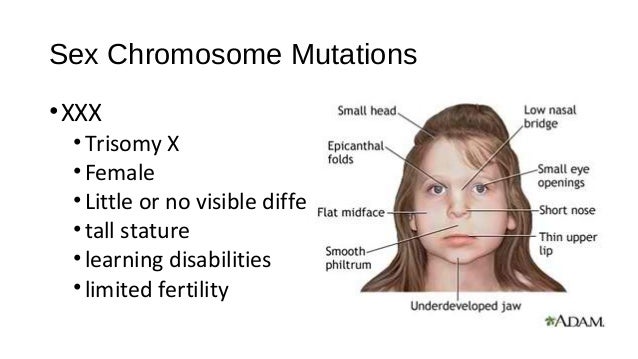
- Physical Features:
- Tall stature
- Hypotonia (reduced muscle tone)
- Hypertelorism (wide-spaced eyes)
- Epicanthal folds (skin fold of the upper eyelid)
- Clinodactyly (curved finger)
- Premature Ovarian Failure (POF) or Primary Ovarian Insufficiency (POI)
- Developmental Delays:
- Speech and/or motor delays
- Learning Disabilities:
- Intellectual disabilities
- Emotional and Behavioral Difficulties:
- Emotional or behavioral challenges
Diagnosis
Diagnosis of trisomy X can be made prenatally through amniocentesis or chorionic villi sampling (CVS). Postnatal diagnosis typically involves karyotyping to confirm the presence of an extra X chromosome. It is important to evaluate for mosaicism and rule out other conditions such as Turner syndrome mosaicism, fragile X, tetrasomy X, and pentasomy X.

Assistive Suggestions and Requirements
Requirement Percentage for Assistive Technology
A significant percentage of individuals with trisomy X may benefit from assistive technology, particularly those with developmental delays and learning disabilities.
Assistive Technology Suggestions
- Communication Aids:
- Speech Generating Devices (SGDs): For individuals with severe speech delays or difficulties.
- Educational Tools:
- Adaptive Learning Software: To support learning and intellectual development.
- Mobility Aids:
- Physical Therapy Equipment: To address hypotonia and improve motor skills.
Access Modalities
- Touchscreen Devices: Useful for individuals with adequate hand dexterity.
- Switch Access: For those with severe motor impairments.
Care Management and Therapeutic Techniques
Aims
- To manage symptoms and support the highest possible level of independence and quality of life.
- To provide multidisciplinary care and address both physical and psychological manifestations.
- To educate and support patients and their families.
SLP Suggestions
- Assessment and Intervention:
- Regular speech and language assessments to monitor progress and adjust therapy plans.
- Techniques to improve speech clarity and language skills.
- Augmentative and Alternative Communication (AAC):
- Introduction of AAC devices early to ensure familiarity and ease of use.
Special Educator Suggestions
- Cognitive Rehabilitation:
- Activities to enhance executive function, memory, and attention.
- Use of memory aids like notebooks or electronic organizers.
- Behavioral Strategies:
- Structured routines to manage emotional and behavioral difficulties.
- Positive reinforcement to encourage participation in educational activities.
Occupational Therapist Suggestions
- Daily Living Skills:
- Training in the use of adaptive equipment for self-care activities.
- Techniques to conserve energy and manage fatigue.
- Home and Environmental Modifications:
- Assessing and modifying the home environment for safety and accessibility.
- Recommendations for ergonomic tools and furniture.
Recommendations on AAC and Other Details
- Text-Based AAC:
- Use of text-to-speech apps and devices for individuals with good literacy skills.
- Predictive text features to speed up communication.
- Symbol-Based AAC:
- For individuals with cognitive impairments affecting literacy, symbol-based systems like Picture Communication Symbols (PCS) can be useful.
- Dynamic display devices that can grow with the user’s needs.
Clinical Information
The following data is from validated clinical sources and patient registries.
Core Characteristics
- Etiology: Genetic
- Pathology: Mutation - De Novo
- Rarity Classification: Medium
- Typical Onset: Birth
- Gender Impact: Women Only
- Seizure Prevalence: Minority (10-50%)
- Population Trend: Stable
Pathophysiology
Reduplication of entire X chromosome; also called "XXX," this is the female variant (in men it would be XXY).
AAC Considerations
Recommended Access Modalities: Touch
Additional Clinical Notes
Estimates indicate only ~10% of Trisomy X cases are ever diagnosed due to lack of symptomaticity. The very small estimate here is based on incidence of language delay and cognitive impact.
Patient Advocacy & Support Organizations
- https://rarediseases.org/rare-diseases/trisomy-x
- www.chromodisorder.org
- https://genetic.org/
Additional Information
Trisomy X is a sex chromosome anomaly with a variable phenotype. The incidence of trisomy X is approximately 1 in 1,000 female births, but only about 10% of cases are clinically ascertained. The phenotype can range from very mild to significant physical and psychological features. Diagnosis can be made prenatally or postnatally through karyotyping. Management requires a multidisciplinary approach, including speech-language pathologists, special educators, and occupational therapists. Support groups and genetic counseling are recommended for affected individuals and their families.
Extended Information
Comprehensive Overview of Trisomy X (47,XXX)
Trisomy X, also known as 47,XXX, is a chromosomal disorder characterized by the presence of an extra X chromosome in females. While typical females have 46 chromosomes, including two X chromosomes (46,XX), individuals with trisomy X have 47 chromosomes, with three X chromosomes (47,XXX). This condition results from a random error during the formation of reproductive cells (eggs and sperm), specifically during the process of meiosis, when chromosomes are supposed to separate evenly. The error, known as nondisjunction, leads to an extra X chromosome in the resulting embryo. Advanced maternal age is a recognized risk factor for nondisjunction events.
Detailed Pathophysiology
The extra X chromosome in trisomy X results in a variable phenotype due to the overexpression of genes that escape X-inactivation. X-inactivation is a normal process in females where one of the X chromosomes in each cell is randomly inactivated to prevent an overdose of X-linked genes. However, some genes on the X chromosome escape inactivation and are expressed from both X chromosomes. In trisomy X, the presence of a third X chromosome means that these escapee genes are overexpressed, contributing to the clinical features of the disorder. The exact genotype-phenotype relationships are not fully understood, and the severity of symptoms can vary widely among affected individuals.
Clinical Presentation
The clinical presentation of trisomy X can vary significantly, ranging from mild to severe. Some individuals may be asymptomatic and never receive a diagnosis, while others may have noticeable physical, developmental, and psychological features. Common physical features include tall stature, hypotonia (reduced muscle tone), hypertelorism (wide-spaced eyes), epicanthal folds (skin fold of the upper eyelid), and clinodactyly (curved finger). Premature ovarian failure (POF) or primary ovarian insufficiency (POI) can also occur, leading to early menopause and infertility.
Developmental and Learning Challenges
Developmental delays are common in trisomy X, particularly in speech and motor skills. Children with trisomy X may experience delays in reaching developmental milestones such as sitting, walking, and talking. Learning disabilities are also prevalent, with some individuals having mild to moderate intellectual disabilities. Difficulties with reading, writing, and mathematics are common, and special educational support may be needed to help these individuals reach their full potential.
Emotional and Behavioral Difficulties
Emotional and behavioral difficulties are frequently reported in individuals with trisomy X. These can include anxiety, depression, and social difficulties. Some individuals may have attention-deficit/hyperactivity disorder (ADHD) or other behavioral challenges. Emotional support and behavioral interventions can be beneficial in managing these difficulties.
Diagnostic Approach
Diagnosis of trisomy X can occur prenatally or postnatally. Prenatal diagnosis is typically made through amniocentesis or chorionic villi sampling (CVS), where fetal cells are analyzed for chromosomal abnormalities. Postnatal diagnosis involves karyotyping, a laboratory technique that visualizes chromosomes to identify the presence of an extra X chromosome. It is important to evaluate for mosaicism, where some cells have the typical 46,XX karyotype and others have 47,XXX, as this can influence the severity of symptoms. Differential diagnosis should rule out other conditions with similar features, such as Turner syndrome mosaicism, fragile X syndrome, tetrasomy X, and pentasomy X.
Therapeutic and Assistive Interventions
Management of trisomy X requires a multidisciplinary approach to address the diverse needs of affected individuals. Speech-language pathologists, special educators, and occupational therapists play crucial roles in supporting development and enhancing quality of life.
Speech-Language Pathology (SLP) Interventions
- Assessment and Intervention: Regular speech and language assessments are essential to monitor progress and adjust therapy plans. Techniques to improve speech clarity and language skills can be beneficial. These assessments should be comprehensive and include a variety of standardized and non-standardized measures to capture the full scope of the individual's abilities and challenges. Intervention strategies might include articulation therapy, language intervention activities, and the use of augmentative and alternative communication (AAC) devices if necessary.
- Augmentative and Alternative Communication (AAC): Introduction of AAC devices early in the treatment process can ensure familiarity and ease of use as the disease progresses. AAC devices can range from simple picture boards to sophisticated speech-generating devices, depending on the individual's needs and abilities. Training both the individual and their caregivers in the use of these devices is crucial for successful communication.
- Family and Caregiver Involvement: Since children spend a large proportion of their time with their caregivers in natural environments outside of the speech-language pathology sessions, there are many opportunities for caregivers to reinforce and facilitate practice of speech and language skills. Activities and everyday conversation and routines can increase the intensity and potentially the effectiveness of speech and language intervention. Caregivers should be provided with strategies and resources to support communication development at home.
- Innovative Service Delivery: In addition to traditional services, innovative forms of service delivery, such as mobile health (mHealth) programs, can be utilized. For example, programs like uTalk in the United States offer mobile-based interventions that can be accessed from home, providing additional support and resources for families.
Special Educator Suggestions
- Cognitive Rehabilitation: Activities designed to enhance executive function, memory, and attention are essential. Special educators can use a variety of techniques to support cognitive development, including the use of memory aids such as notebooks or electronic organizers. Structured routines and visual schedules can help manage time and tasks effectively.
- Behavioral Strategies: Implementing structured routines to manage emotional and behavioral difficulties is crucial. Positive reinforcement can encourage participation and effort in educational activities. Behavioral interventions should be individualized based on the child's specific needs and challenges.
- Educational Support: Special educators should work closely with the family and other professionals to develop an individualized education plan (IEP) that addresses the child's unique needs. This plan should include specific goals and strategies for supporting speech, language, and cognitive development within the educational setting.
Occupational Therapist Suggestions
- Daily Living Skills: Training in the use of adaptive equipment for self-care activities (e.g., dressing, grooming) is essential. Occupational therapists can provide strategies to conserve energy and manage fatigue, ensuring that the individual can participate in daily activities as independently as possible.
- Home and Environmental Modifications: Assessing and modifying the home environment to ensure safety and accessibility is a key role of occupational therapists. Recommendations for ergonomic tools and furniture can support independence and reduce physical strain.
- Sensory Integration Therapy: For individuals with sensory processing difficulties, sensory integration therapy can help improve the ability to process and respond to sensory information. This therapy can be particularly beneficial for addressing challenges with motor skills and coordination.
Recommendations on AAC and Other Details
- Text-Based AAC: Use of text-to-speech apps and devices for individuals with good literacy skills can facilitate communication. Predictive text features can speed up communication and reduce the effort required to type out messages.
- Symbol-Based AAC: For individuals with cognitive impairments affecting literacy, symbol-based systems like Picture Communication Symbols (PCS) can be useful. Dynamic display devices that can grow with the user’s needs offer flexibility and adaptability as the individual's communication skills develop.
- Voice and Communication Modifications: SLPs can help patients safely modify their voice and communication behaviors, including verbal and nonverbal communication. This includes interventions to improve vocal pitch, intonation, voice quality, resonance, fluency, articulation, pragmatics, and vocalization (e.g., laughing). These interventions should be evidence-based and focused on achieving patient-specific functional goals.
References
- Tartaglia, N. R., Howell, S., Sutherland, A., Wilson, R., & Wilson, L. (2010). A review of trisomy X (47,XXX). Orphanet Journal of Rare Diseases, 5(8). Link
Additional Information
Trisomy X is a sex chromosome anomaly with a variable phenotype. The incidence of trisomy X is approximately 1 in 1,000 female births, but only about 10% of cases are clinically ascertained. The phenotype can range from very mild to significant physical and psychological features. Diagnosis can be made prenatally or postnatally through karyotyping. Management requires a multidisciplinary approach, including speech-language pathologists, special educators, and occupational therapists. Support groups and genetic counseling are recommended for affected individuals and their families.
State and Federal Advocacy
It is important for families and healthcare providers to stay informed about state and federal advocacy efforts related to trisomy X and other genetic conditions. Advocacy can help improve access to services, funding for research, and public awareness. Engaging in advocacy efforts can also provide families with a sense of community and support.
In conclusion, trisomy X is a complex condition that requires a comprehensive, multidisciplinary approach to management. Early diagnosis and intervention, along with ongoing support from healthcare professionals, educators, and caregivers, can significantly improve the quality of life for individuals with trisomy X.
Epidemiology and Demographics
Etiology and Pathophysiology
What causes Trisomy X?
What does Trisomy X do to the body?
Clinical Features and Stages
Diagnosis
Diagnostic Criteria
Genetic Testing
Differential Diagnosis
Assistive Technology and AAC Interventions
Communication Devices
Mobility Aids
Access Modalities
Environmental Control Units
Clinical Recommendations
For Speech-Language Pathologists
For Occupational Therapists
For Physical Therapists
For Applied Behavior Analysts
For Special Educators
For All Staff and Caregivers
Care Management
Medical Management
Positioning and Handling
Feeding and Swallowing
Psychosocial Support
Educational Support
IEP Goal Examples
Accommodations and Modifications
Transition Planning
Support and Resources
🏛️ Foundations and Research
🌐 Online Communities
📚 Educational Resources
💰 Financial Assistance
References
Disclaimer: This comprehensive clinical guide is designed for healthcare professionals, educators, and families. For specific medical advice, please consult with qualified healthcare providers.